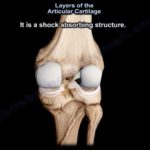
Courtesy: Justin Arner MD, Associate Professor, University of Pittsburgh, Pennsylvania, USA Meniscus Anatomy and Function The medial meniscus is C-shaped; the lateral meniscus is more U-shaped and mobile. Composed primarily of: Type I collagen (predominantly peripheral) Type II collagen (more central) High water content Glycosaminoglycans Functions: Load transmission Shock absorption Stability Lubrication Proprioception Vascular Zones […]
MPFL reconstruction

Courtesy: Dr Strickland, Ashok Shyam TV, Ortho Background and Evolution of Treatment Medial patellofemoral ligament reconstruction was rarely performed two decades ago. The ligament was historically under-recognized in patellar instability. Over the last 12 to 13 years, understanding of its importance has significantly increased. Patellar instability can lead to: Loss of athletic participation for an […]
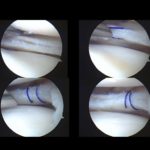
Lateral meniscus root repair
Courtesy: Dr Ranawat, Ashok Shyam TV, Ortho Evolution in Meniscus Root Management Meniscus root repair represents a major advancement in knee preservation surgery. The medial root has transformed arthritis prevention strategies. The lateral root is increasingly recognized as critical for knee stability, particularly in anterior cruciate ligament–deficient knees. Modern sports medicine now emphasizes identifying and […]
MPFL Repair-Graft Position

Courtesy: Dr B Sabnis, Ashok Shyam TV, Ortho MPFL Anatomy Overview The medial patellofemoral ligament (MPFL) is a fan-shaped structure. Length varies with body habitus: Approximately 46–49 mm in smaller Asian populations. Approximately 50–56 mm in Caucasian populations. Indian population typically in between. Width ranges widely (3–30 mm), consistent with its fan-shaped configuration. Patellar Attachment […]
Patellofemoral cartilage repair
Courtesy: Dr A Gomoll, Ashok Shyam TV, Ortho Clinical Context First-time patellar dislocators traditionally require surgery only when a loose body is present. However, many patients present with: Cartilage defects on magnetic resonance imaging. No loose body. Unclear indication for surgery. Key question:When should patellofemoral cartilage defects be treated surgically? Incidence of Patellofemoral Cartilage Defects […]
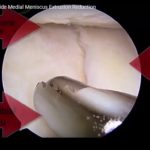
Medial meniscus root repair
Courtesy: Dr Strickland, Ashok Shyam TV, Ortho Changing Perspective Repair of medial meniscus root tears has gained momentum only in the last several years. Historically, many of these tears—especially in middle-aged patients—were treated nonoperatively or with meniscectomy. These are sometimes referred to as “underserved tears” because they were frequently missed or undertreated. The key questions: […]
Templating in THR

Courtesy: Dr T Vail, Ashok Shyam TV, Ortho 1?? Evaluation of Labral Pathology and Femoroacetabular Impingement Patient Counseling and Expectations When evaluating patients with: Labral tears Femoroacetabular impingement Key counseling points include: Recovery Timeline Simple labral debridement: Recovery approximately 6 weeks. Extensive impingement correction (cam/pincer correction, labral repair): Recovery 4 to 6 months. Recovery after […]
Hip Imaging Radiograph and MRI
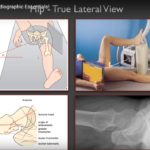
Courtesy: Dr T Vail, Ashok Shyam TV, Ortho Why Hip Imaging Matters Imaging plays a critical role in: Understanding hip biomechanics Planning hip reconstruction procedures Identifying intra-articular pathology Direct visualization (e.g., arthroscopy) highlights how challenging it can be to detect subtle pathology using imaging alone. Each modality (plain radiographs, MRI) has specific strengths and limitations. […]
Cementless THR

Courtesy: Dr D Padgett, Ashok Shyam TV, Ortho Limitations of Cemented Fixation Cement fatigue fractures may: Lead to implant loosening Contribute to particle-induced osteolysis Certain patient groups historically performed poorly with cemented fixation: Heavy, highly active males Ideal goal: Direct bone–implant fixation Avoidance of an intermediary cement layer Elimination of a second mechanical interface Biologic […]
Current Trends in Hemi Arthroplasty

Courtesy: Dr Suryanaraya, Ashok Shyam TV, Ortho Hemiarthroplasty vs Total Hip Arthroplasty in the Elderly Ongoing debate in displaced femoral neck fractures: Internal fixation vs hemiarthroplasty vs THA. Considerations: Functional outcome Morbidity and mortality Revision risk Historical Failures of Early Hemiarthroplasty Primary Causes of Early Failure Metallurgical failure Fixation failure Cartilage degeneration over time Design-Related […]
Hip-Alternate Bearing Ceramic
Courtesy: Dr C Ranawat, Ashok Shyam TV, Ortho
Osteolysis in TKR

Courtesy: Dr Ranawat, Ashok Shyam TV, Ortho Background Osteolysis remains a significant long-term complication in total knee arthroplasty (TKA). Strongly associated with: Polyethylene wear debris Modular implant designs Historically uncommon in: Fixed-bearing, monoblock all-polyethylene tibial components. Historical Perspective All-Polyethylene Fixed-Bearing Knees Single-unit tibial component. Long-term data (up to 20+ years): Minimal to no osteolysis reported. […]
Painful and Stiff Knee

Courtesy: Dr T Vail, Ashok Shyam TV, Ortho Overview TKA is successful in ~95% of patients. The remaining 2–5%: Experience pain, stiffness, or dissatisfaction. Often consume a disproportionate amount of clinical time. Typical scenario: Radiographs appear normal. Patient reports the knee “just doesn’t feel right.” Clinical Presentation Patients may report: Stiffness Swelling Limited flexion […]
Mobile Bearing TKR

Courtesy: Dr Maniar, Ashok Shyam TV, Ortho Why Consider a Mobile-Bearing Knee? Primary concern: Polyethylene wear: At the articular surface At the undersurface (backside wear) Fixed-bearing knees have demonstrated: Significant articular wear. Undersurface micromotion leading to wear debris. Associated osteolysis and revision in mid-term follow-up. Problem 1: Articular Surface Wear Contact Stress Principle Contact stress […]
Cruciate Retaining TKR

Courtesy: Dr A Reddy, Ashok Shyam TV, Ortho Introduction Focus: Cruciate-retaining (CR) total knee arthroplasty. Personal practice preference: ~99% of primary TKAs performed as CR knees. Used even in severe deformities. Transition from posterior-stabilized (PS) to CR: Smaller knee sizes. Thinner femoral condyles. Concerns regarding box cuts in smaller bone stock. Why Choose Cruciate Retaining? […]