Corutesy: Dr Amr Abdelgawad, Texas tech University, El Paso, Texas, USA
Distal Radius Fractures in Children
1. Normal Wrist X-ray Anatomy
Essential Views
- AP view
- Lateral view
Key Bony Structures
- Radius – primary articular bone
- Ulna – smaller, less involved in articulation
Physis (Growth Plate)
- Smooth, regular line
- Indicates skeletal immaturity
- Must not be mistaken for a fracture
Carpal Landmarks
- Scaphoid
- Lunate
2. Types of Distal Radius Fractures
A. Torus (Buckle) Fracture
Definition
- Incomplete fracture due to compression
- Causes buckling of one cortex
Features
- Stable fracture
- No complete cortical disruption
- Common in younger children
X-ray Findings
- Subtle cortical bulge
- Best seen on lateral view
Treatment
- Removable splint or short cast
- No reduction required
- No repeat X-ray needed
B. Metaphyseal Fracture
Definition
- Complete fracture through metaphysis
Types
- Undisplaced
- Displaced
Features
- May involve radius ± ulna
- Visible deformity if displaced
Treatment
- Closed reduction + casting
- If unstable – K-wire fixation
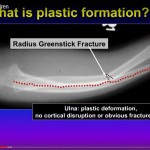
C. Greenstick Fracture
Definition
- Incomplete fracture with angulation
- One cortex breaks, opposite cortex bends
Features
- Angulated deformity
- Common due to bone elasticity
Treatment
- Closed reduction
- Cast immobilization
D. Physeal Injury (Salter–Harris Classification)
Basic Anatomy
- Diaphysis – Metaphysis – Physis – Epiphysis
Salter–Harris Types
| Type | Description | Key Point |
|---|---|---|
| I | Through physis | Epiphysis separated |
| II | Physis + metaphysis | Most common |
| III | Physis + epiphysis | Intra-articular |
| IV | Metaphysis + physis + epiphysis | Growth risk |
| V | Crush injury | Poor prognosis |
Type II – Key Details
- Most common type
- Features:
- Metaphyseal fragment
Thurston–Holland Fragment
- Triangular metaphyseal fragment
- Diagnostic clue
Treatment Principles
- Gentle reduction
- Avoid forceful manipulation
- Accept minor deformity (high remodeling potential)
3. Management Principles
General Assessment
- Neurovascular status
- Examine entire limb
Treatment Summary
| Fracture Type | Treatment |
|---|---|
| Torus | Splint |
| Greenstick | Reduction + cast |
| Metaphyseal displaced | Reduction ± K-wire |
| Salter-Harris | Gentle reduction |
4. Important Clinical Pearls
1. Always Examine Entire Limb
- Wrist injury – assess elbow
Must Not Miss
- Monteggia fracture
2. Radiological Rule
- X-ray:
- Joint above and below
3. Growth Plate Protection
- Avoid aggressive manipulation
- Risk:
- Growth arrest
4. Remodeling Potential
- High in children
- Mild deformity often acceptable
5. Red Flags for Orthopaedic Referral
- Displaced fractures
- Physeal injuries
- Neurovascular compromise
- Associated injuries
- Failed reduction
6. Quick Exam Summary
- Torus – Stable – Splint
- Greenstick – Angulated – Reduce + Cast
- Metaphyseal – Complete – Reduce ± K-wire
- Salter-Harris II – Most common – Gentle reduction

Thanks a lot for this valuable lecture