Courtesy: Kaye WIlkins MD
Lynn Staheli MD
Terminology
Preferred terminology
- Fracture of the shaft (diaphysis) of the radius and or ulna.
- Avoid the vague term “both bone forearm fracture.”
Epidemiology
Age distribution
- Boys commonly sustain injuries at 9 to 10 years due to playground activities.
- A second peak occurs at 14 to 15 years due to sports injuries.
- Girls traditionally have an earlier peak, although this is changing with increased sports participation.
Anatomical Distribution
Location of fractures
- Metaphyseal fractures account for approximately 52 percent.
- Distal physeal and metaphyseal fractures account for approximately 70 percent.
- Shaft fractures account for approximately 25 percent.
- Proximal fractures account for approximately 6 percent.
Distribution within shaft fractures
- Proximal third: Approximately 9 percent.
- Middle third: Approximately 30 percent.
- Distal third: Approximately 57 percent.
Reasons distal shaft fractures are more common
- Weaker metaphyseal transition zone.
- Less muscle protection.
- Longer lever arm.
Muscle Forces and Deforming Forces
Proximal fragment
- Biceps produces flexion and supination.
- Supinator produces supination and external rotation.
Distal fragment
- Pronator teres and pronator quadratus produce pronation.
- Brachioradialis causes shortening and angulation.
Clinical importance
- Muscle forces create rotational malalignment after fracture.
Classification
Based on fracture level
- Proximal third.
- Middle third.
- Distal third.
Based on fracture completeness
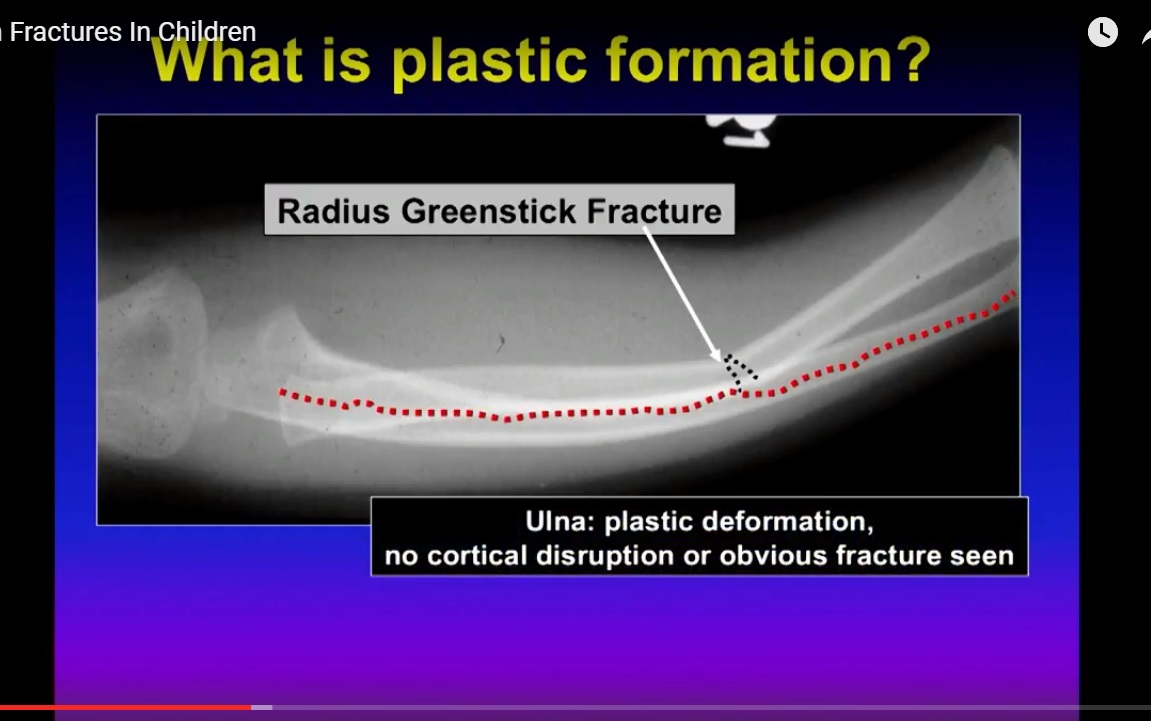
- Plastic deformation.
- Greenstick fracture.
- Complete fracture.
Based on deformity
- Angulation.
- Rotation.
Types of Fractures
Plastic deformation
- No cortical break.
- Permanent bending due to internal structural failure.
- Presents with forearm deformity and loss of pronation and supination.
- Pain may be minimal.
Greenstick fracture
- Tension cortex is fractured.
- Compression cortex remains intact.
- Most commonly presents with supination and apex volar deformity.
- Less commonly presents with pronation and apex dorsal deformity.
- Both rotational and angular deformities must be corrected.
Complete fracture
- Both cortices are disrupted.
- Associated with shortening, angulation, and rotational deformity.
Principles of Reduction
General principle
- Correct rotational deformity first.
- Correction of angulation often follows automatically.
Reduction according to deformity
- Supination with apex volar deformity: Pronate the forearm.
- Pronation with apex dorsal deformity: Supinate the forearm.
Treatment
Plastic deformation
- Gradual sustained pressure over a fulcrum.
- Goal is restoration of forearm rotation rather than perfect radiographs.
- Immobilize for approximately 6 weeks.
Greenstick fracture
- Closed reduction followed by casting.
- Completion of the fracture remains controversial.
- Completing the fracture may improve callus formation and reduce refracture risk.
- It may also increase instability and hematoma formation.
Complete fracture
- Closed reduction and casting if acceptable alignment is achieved.
Principles of Casting
- Long arm cast is usually preferred.
- Cast position should be determined by the fracture pattern rather than the fracture level.
Older teaching
- Distal fractures in pronation.
- Midshaft fractures in neutral.
- Proximal fractures in supination.
Current concept
- Cast according to the deformity and reduction achieved.
Cast in extension (Rang technique)
- Useful when there is a high risk of redisplacement.
- May be used after remanipulation.
- Include the thumb to prevent cast slippage.
Acceptable Reduction (Price Criteria)
Children younger than 9 years
- Angulation up to 15 degrees.
- Rotation up to 45 degrees.
Children older than 9 years
- Angulation up to 10 degrees.
- Rotation up to 30 degrees.
Shortening
- Less than 1 cm is acceptable.
Indications for Surgery
- Open fractures.
- Compartment syndrome.
- Failure of closed reduction.
- Inability to maintain reduction.
- Ipsilateral injuries such as floating elbow.
- Refractures.
- Severe soft tissue injury.
Surgical Options
Intramedullary nailing
- Preferred method using elastic nails or Kirschner wires.
- Causes minimal soft tissue damage.
- Shorter operative time.
- Easier implant removal.
Plate fixation
- Useful in selected fractures.
External fixation
- Reserved for severe soft tissue injury or complex trauma.
Special Situations
Refracture
- Occurs in approximately 10 percent.
- Risk factors include early return to activity, greenstick fractures, and residual deformity.
- Often treated with intramedullary nailing.
Floating elbow
- Fix the forearm fracture first to improve leverage during reduction.
Rotational malalignment
- Compare the radial tuberosity with the radial styloid.
- Normal relationship is approximately 180 degrees.
- Rotational deformity is commonly overlooked.
Complications
- Loss of reduction.
- Malunion.
- Refracture.
- Radioulnar synostosis.
- Compartment syndrome.
- Nerve injury.
Exam Pearls
- Rotational alignment is more important than angular alignment.
- The proximal fragment is the “king fragment” because it determines reduction.
- Greenstick fractures have both rotational and angular deformities.
- Plastic deformation is easily missed.
- Diaphyseal fractures have less remodeling potential than distal forearm fractures.
Leave a Reply