Courtesy: Prof Nabil Ebraheim, University of Toledo, Ohio, USA
Pediatric Femoral Shaft Fractures
Overview
Pediatric femoral shaft fractures
- One of the most common causes of pediatric orthopedic hospitalization.
- Management depends on age, fracture pattern, fracture location, and the child’s weight.
Age Based Treatment Algorithm
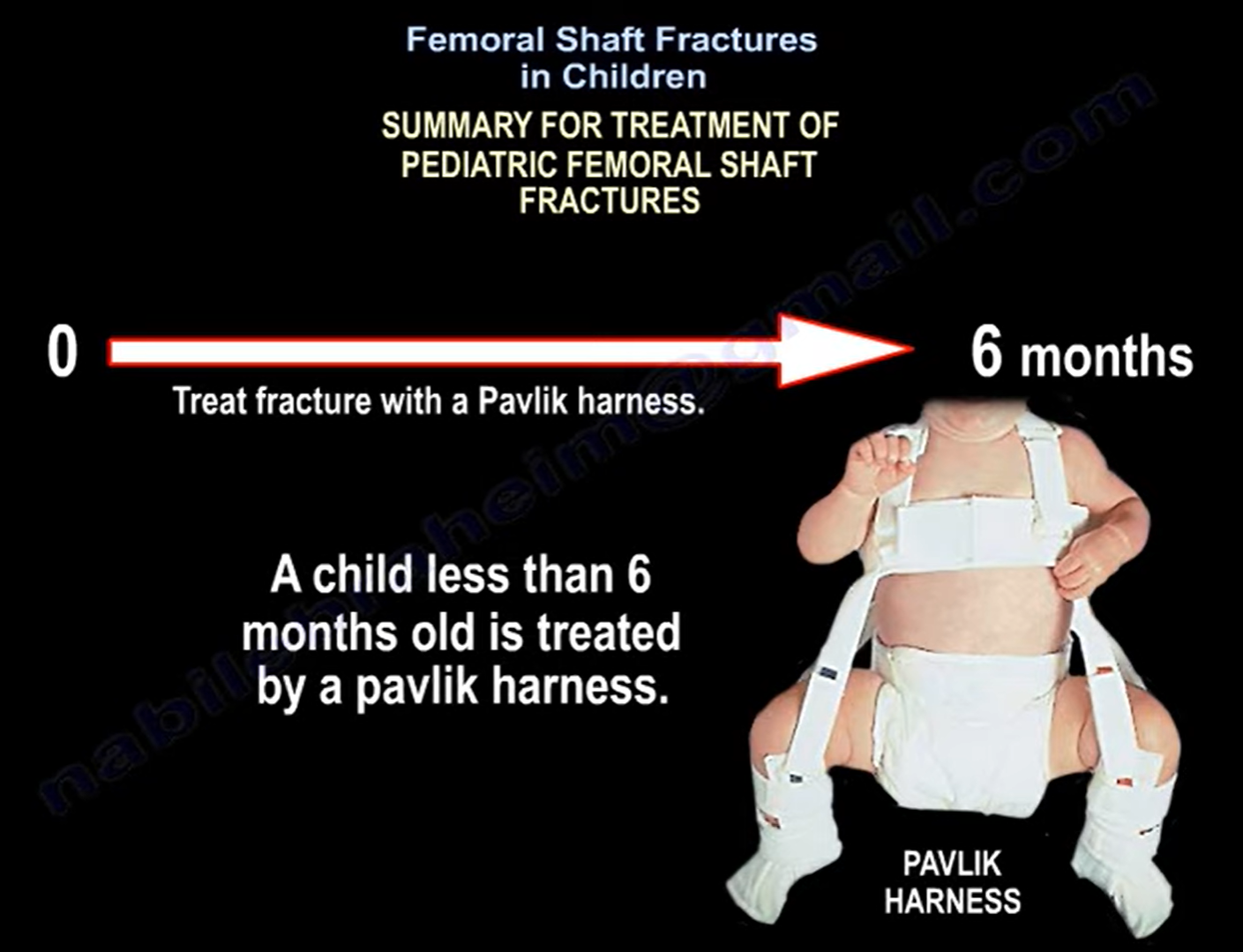
Less than 6 months
- Pavlik harness.
6 months to 5 years
- Closed reduction and hip spica cast.
- Acceptable shortening is up to 2 cm.
- Shortening greater than 2 to 3 cm may require traction followed by delayed spica casting, although this is rarely used today.
- Avoid the 90 90 spica position because of the risk of compartment syndrome.
Special consideration
- Femoral shaft fracture in a non ambulatory child younger than 2 years should raise suspicion for non accidental trauma.
- Transverse fractures are particularly concerning.
5 to 11 years
- Operative management is usually preferred.
Flexible intramedullary nailing
- Best for diaphyseal transverse or short oblique fractures.
- Suitable for children younger than 11 years weighing less than 45 kg.
- Use two nails with a combined diameter equal to approximately 80 percent of the femoral canal.
- Most common complication is knee irritation at the entry site.
- Avoid in children older than 11 years, weighing more than 45 to 50 kg, or with length unstable fractures.
Submuscular plating
- Preferred for comminuted fractures.
- Suitable for proximal and distal shaft fractures.
- Bridge plating technique is commonly used.
- Aim for three screws proximal and three screws distal whenever possible.
External fixation
- Indicated for open fractures.
- Useful for polytrauma as damage control.
- Complications include knee stiffness and refracture after fixator removal.
Older than 12 years
- Rigid intramedullary nail.
- Submuscular plating when indicated.
Entry Point for Intramedullary Nailing
Preferred entry
- Lateral greater trochanter.
Avoid
- Piriformis fossa.
Reason
- Risk of injury to the medial femoral circumflex artery.
- May result in avascular necrosis of the femoral head.
Complications
Leg length discrepancy
- Most common complication.
- Usually due to overgrowth.
- Common in children younger than 10 years.
- Typically 0.5 to 2 cm.
- Occurs within the first two years after injury.
Loss of reduction in hip spica
- Risk increases with increasing initial shortening.
- One cm shortening has approximately 12 percent risk.
- Two cm shortening has approximately 24 percent risk.
- Three cm shortening has approximately 50 percent risk.
Malalignment
- More common after flexible intramedullary nailing.
- Up to 15 degrees of angulation may be acceptable depending on age.
Compartment syndrome
- Reduced by applying the body portion of the spica cast before the limb portion.
Traction pin complications
- Proximal tibial traction pins may cause tibial tubercle growth arrest.
- May result in genu recurvatum.
External fixation
- Increased risk of refracture after fixator removal.
Exam Pearls
- Less than 6 months: Pavlik harness.
- 6 months to 5 years: Hip spica cast.
- 5 to 11 years: Flexible intramedullary nails for length stable fractures.
- Comminuted or length unstable fractures: Submuscular plating.
- Open fractures or polytrauma: External fixation.
- Older than 12 years: Rigid intramedullary nail using a lateral greater trochanteric entry.
- Piriformis entry increases the risk of avascular necrosis of the femoral head.
- Most common complication is leg length discrepancy due to overgrowth.
- Flexible nails should not be used for length unstable fractures or in heavier children.
Key Take Home Message
- Treatment depends on age, fracture stability, fracture pattern, and patient size.
- Always assess length stability before selecting fixation.
- Lateral trochanteric entry is the preferred approach for rigid intramedullary nailing in adolescents.
- Most children heal well with appropriate treatment, but careful attention to alignment and limb length is essential for optimal outcomes.


Leave a Reply