Courtesy: Prof Nabil Ebraheim, University of Toledo, Ohio, USA
Pediatric Femoral Shaft Fractures
Overview
Pediatric femoral shaft fractures are among the most common major orthopedic injuries in children.
Management primarily depends on:
- Age of the child
- Fracture pattern
- Stability of fracture
- Weight of the child
- Associated injuries
Important Clinical Red Flag
A femoral shaft fracture in a non-ambulatory child should raise strong suspicion for:
- Non-accidental trauma (child abuse)
Particularly concerning features include:
- Inconsistent history
- Delay in presentation
- Multiple fractures
- Associated injuries
Deforming Forces
Understanding muscle forces helps predict fracture displacement.
Proximal Fragment
Typical deformities:
- Flexion
- External rotation
- Abduction
Muscles responsible:
- Iliopsoas
- Hip abductors
Distal Fragment
Typical deformity:
- Shortening
Muscles responsible:
- Hamstrings
- Quadriceps
These muscles are biarticular and generate significant shortening forces.
Age-Based Treatment Algorithm
Infants (0–6 Months)
Preferred Treatment
Pavlik Harness
Advantages:
- No anesthesia required
- Easier nursing care
- Allows parental bonding
- Excellent remodeling potential
Disadvantages:
- Less rigid stabilization
- Initial muscle spasm possible
Children (6 Months–5 Years)
Gold Standard
Early Hip Spica Cast
Best suited for:
- Stable fractures
- Shortening less than 2 cm
Contraindications to Early Spica
Avoid isolated spica casting in:
- Unstable fractures
- Shortening greater than 2–3 cm
- High-energy injuries
Alternative Options
- Traction followed by delayed spica
- External fixation in selected cases
Proper Spica Positioning
Correct positioning is critical.
Recommended position:
- Hip flexion: 30–40°
- Hip abduction with external rotation
- Knee flexion: approximately 30°
Purpose:
- Relaxes iliopsoas
- Relaxes hamstrings
- Reduces shortening forces
Improper “anatomical” positioning may result in:
- External rotation deformity
- Angulation
- Persistent shortening
Complications of Spica Casting
- Loss of reduction
- Malalignment
- Shortening
- Skin complications
- Compartment syndrome
Close follow-up is essential.
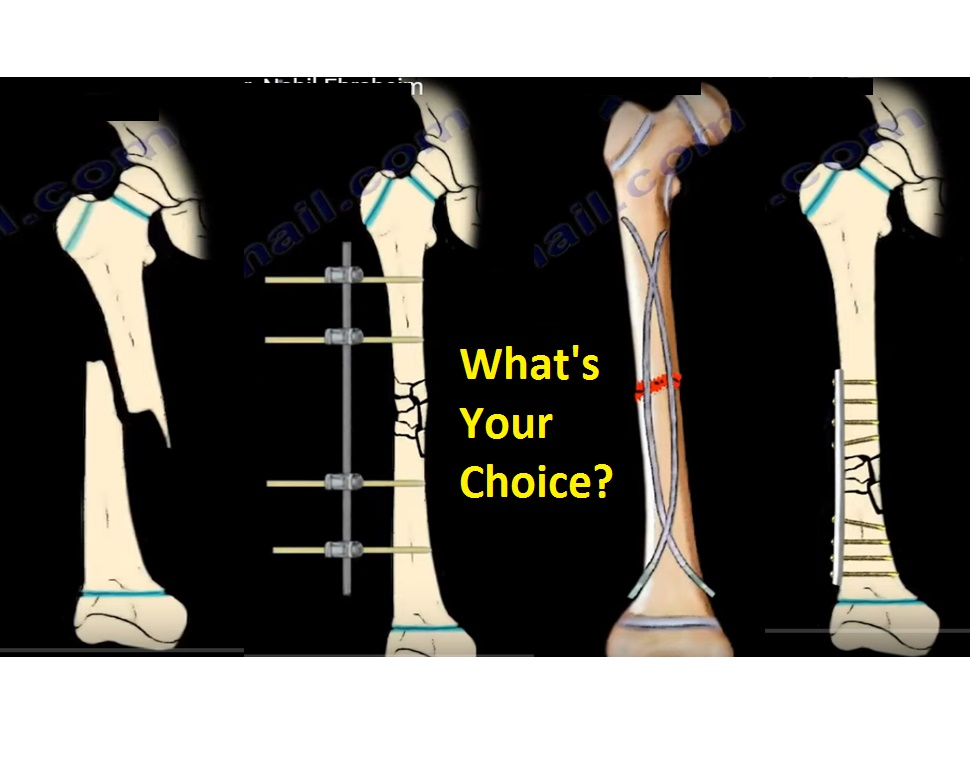
Children (5–11 Years)
Multiple treatment options exist.
1. Flexible Intramedullary Nails (TENs / ESIN)
Most commonly used technique in this age group.
Indications
- Age 5–11 years
- Weight less than approximately 45 kg
- Midshaft fractures
- Transverse fractures
- Short oblique fractures
Not Ideal For
- Comminuted fractures
- Length-unstable fractures
- Very proximal fractures
- Very distal fractures
Biomechanical Principle
Pre-bent elastic nails provide:
- Three-point fixation
- Relative stability
- Controlled micromotion
Nail Size
Recommended diameter:
- Approximately 0.4 × medullary canal diameter
Goal:
- About 80% canal fill
Technique Points
- Nails should be pre-bent
- Usually inserted retrograde
- Rotation must be checked clinically after fixation
Complications
- Malalignment
- Shortening
- Nail migration
- Skin irritation
Up to 15° malalignment may occur.
Preventing Shortening
Options include:
- End caps
- Third nail
- Alternative fixation methods
2. Submuscular Plating
Useful for unstable fracture patterns.
Indications
- Comminuted fractures
- Length-unstable fractures
- Proximal fractures
- Distal fractures
- Heavier children (>45 kg)
Advantages:
- Better alignment control
- Suitable for difficult fracture patterns
3. External Fixation
Indications
- Open fractures
- Polytrauma
- Vascular injury
- Severe soft tissue injury
Major Complication
- Refracture after fixator removal
Adolescents (>11 Years / Near Skeletal Maturity)
Options
- Rigid intramedullary nail
- Plate fixation
- External fixation
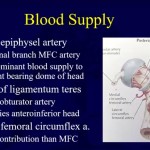
Intramedullary Nailing
Important Surgical Principle
Avoid piriformis entry nails in children.
Reason
Risk of injury to:
- Medial femoral circumflex artery
This may lead to:
- Avascular necrosis (AVN) of femoral head
Preferred Entry Point
Greater Trochanteric Entry
Safer regarding femoral head blood supply.
Possible complications:
- Coxa valga
- Premature greater trochanter apophyseal closure
Skeletally Mature Adolescents
Adult-style antegrade intramedullary nailing may be used.
Traction
Now less commonly used.
Types
- Skin traction
- Skeletal traction
Limitations
- Prolonged hospitalization
- Muscle wasting
- Skin problems
- Difficult nursing care
Complications of Pediatric Femoral Shaft Fractures
1. Limb Length Discrepancy (Most Common)
Typically due to overgrowth.
Characteristics:
- More common in children <10 years
- Usually develops within 2 years
- Overgrowth may reach approximately 2 cm
Acceptable shortening at presentation:
- Up to 2 cm
2. Malunion
More common with:
- Flexible nails
- Inadequate reduction
3. Compartment Syndrome
May occur after:
- Spica casting
- High-energy trauma
Requires urgent recognition.
4. Refracture
Especially after:
- External fixator removal
5. Avascular Necrosis of Femoral Head
Associated with:
- Piriformis entry nails
6. Growth Disturbance
May occur from traction pin placement.
Example:
- Proximal tibial traction pin causing recurvatum deformity
Key Exam Pearls
- 0–6 months: Pavlik harness
- 6 months–5 years: Early spica cast
- 5–11 years: Flexible nails for stable fractures
- Older children/adolescents: Rigid fixation methods
- Avoid piriformis entry in children due to AVN risk
- Most common complication: Limb length discrepancy
- Femur fracture in non-walking child should prompt evaluation for child abuse

Leave a Reply