Courtesy: Prof Nabil Ebraheim, University of Toledo, Ohio, USA
Introduction
Calcaneal fractures are associated with a high risk of soft tissue complications because the heel has a thin soft tissue envelope and limited vascularity.
The condition of the skin and soft tissues often determines:
- Timing of surgery
- Choice of surgical approach
- Final outcome
High Risk Fracture Patterns
The following injuries can rapidly compromise the skin:
Displaced Tuberosity Fractures
- Posterior fragment displaced by Achilles tendon pull
- Can cause skin tenting and necrosis
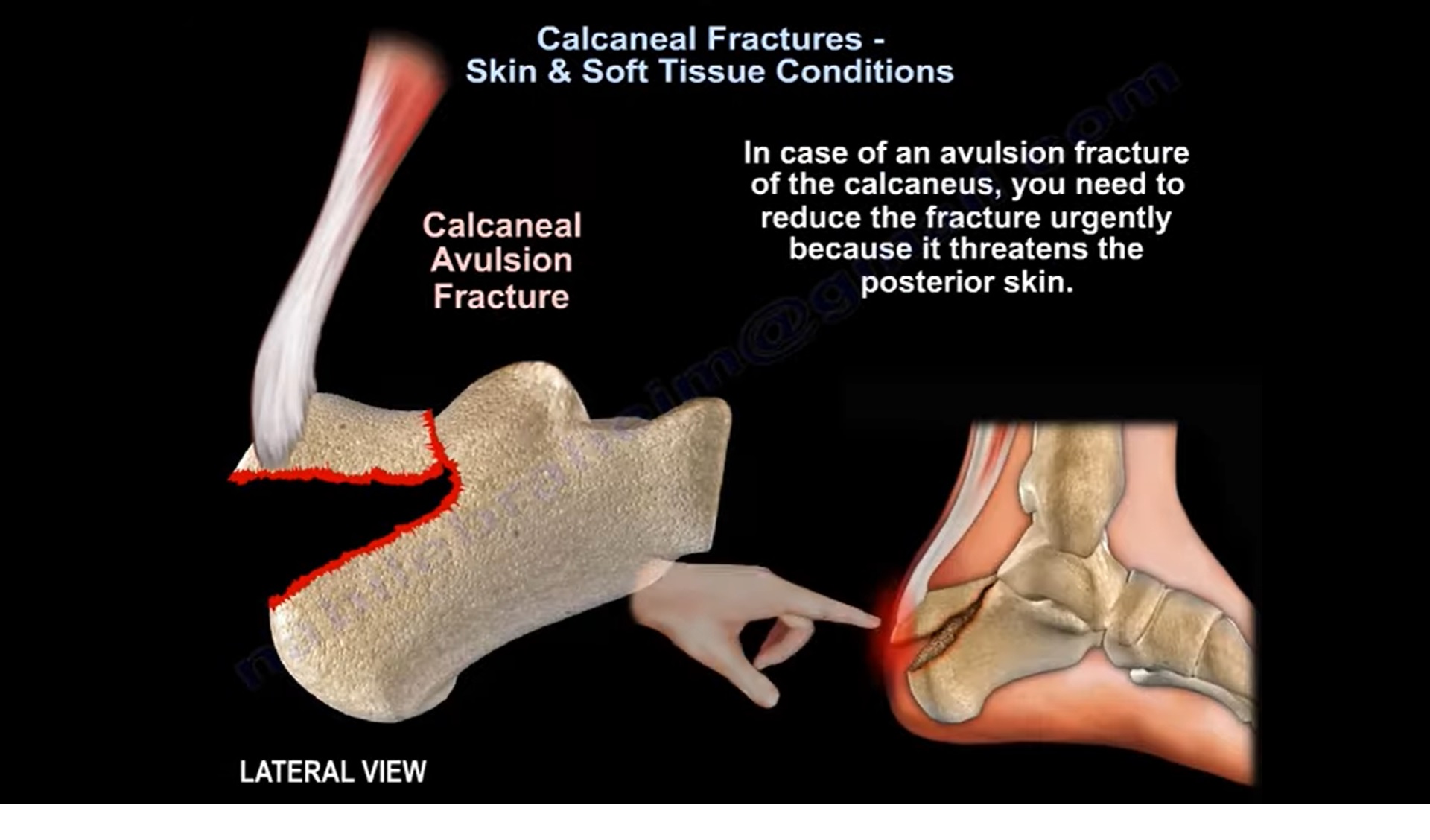
Avulsion Fractures
- Frequently seen in diabetic patients
- Posterior skin may become ischemic
Tongue Type Calcaneal Fractures
- Posterior fragment displaced superiorly
- Direct pressure on posterior heel skin
- Risk of full thickness skin necrosis
Tongue Type Fractures
Why They Are Important
The displaced posterior fragment presses directly against the heel skin.
Consequences:
- Skin blanching
- Skin necrosis
- Wound breakdown
- Exposure of bone
Management
These fractures are considered an orthopedic emergency.
Treatment:
- Urgent reduction
- Percutaneous fixation whenever possible
Clinical Pearl
Do not wait for soft tissue swelling to settle in a severely displaced tongue type fracture.
Avulsion Fractures of the Calcaneal Tuberosity
Characteristics
- Achilles tendon pulls the fragment proximally
- Posterior skin becomes stretched
High Risk Patients
- Diabetics
- Elderly patients
- Peripheral vascular disease
Management
Urgent reduction and fixation are required.
Delay may result in:
- Full thickness skin necrosis
- Soft tissue loss
- Infection
Operative Versus Non Operative Treatment
For displaced intraarticular fractures:
Advantages of Surgery
- Better restoration of anatomy
- Reduced risk of subtalar arthritis
- Improved function in selected patients
Some studies suggest:
- Younger patients
- Particularly younger women
may achieve better outcomes with surgery.
Wound Complications
The most common complication after calcaneal surgery is wound related.
Common Problems
Delayed Wound Healing
Most frequent complication.
Wound Dehiscence
- Breakdown of wound edges
- Exposure of implants
Infection
Superficial Infection
Relatively common.
Deep Infection
Occurs in approximately 1 to 4% of closed fractures.
Risk Factors for Wound Problems
Major risk factors include:
- Smoking
- Diabetes mellitus
- Peripheral vascular disease
- Poor circulation
- Severe soft tissue swelling
- Open fractures
These patients may be better managed non operatively.
Fracture Severity and Complications
Sanders Type IV Fractures
Associated with:
- Greater articular destruction
- More soft tissue injury
- Higher complication rates
- Worse outcomes
Surgical Approaches
Extended Lateral Approach
Historically the most common approach.
Advantages
- Excellent visualization
- Direct reduction of fracture
Disadvantages
- High wound complication rate
- Delayed healing
- Wound necrosis
Reported Complication Rate
Delayed wound healing may occur in up to 20% of patients.
Sinus Tarsi Approach
Increasingly popular.
Advantages
- Smaller incision
- Better soft tissue preservation
- Lower wound complication rate
Disadvantages
- Limited visualization in highly comminuted fractures
Timing of Surgery
General Principle
Delay surgery until soft tissues recover.
Wrinkle Test
Presence of skin wrinkles indicates readiness for surgery.
Absence of wrinkles indicates significant swelling and increased risk of wound complications.
Exceptions Requiring Urgent Surgery
Displaced Tongue Type Fracture
Calcaneal Tuberosity Avulsion Fracture
Reason:
- Imminent risk of posterior skin necrosis
Compartment Syndrome of the Foot
Incidence
Occurs in up to 10% of severe calcaneal fractures.
Why It Occurs
The plantar fascia restricts expansion of foot compartments.
Increasing pressure causes:
- Muscle ischemia
- Nerve injury
Consequences
If untreated:
- Intrinsic muscle contracture
- Clawing of toes
- Chronic pain
- Difficulty wearing footwear
Treatment
Emergency fasciotomy.
Foot Compartments
There are nine compartments:
Medial
- 1 compartment
Lateral
- 1 compartment
Interosseous
- 4 compartments
Adductor
- 1 compartment
Central
- Superficial central compartment
- Deep central compartment
Open Calcaneal Fractures
Characteristics
Associated with:
- High infection rates
- Soft tissue loss
- Amputation risk
Surgical Considerations
Grade III Medial Open Fractures
Generally not suitable for ORIF.
Most Lateral Open Fractures
Also have high complication rates with ORIF.
Risks
- Infection
- Osteomyelitis
- Wound breakdown
- Amputation
Selected Grade I and II Medial Open Fractures
May be treated surgically with:
- Thorough debridement
- Stable fixation
- Appropriate soft tissue management
In carefully selected cases:
- Infection rates may approach those of closed fractures.
Antibiotic Protocol
Typically:
- Intravenous antibiotics
- Continued for 2 to 3 days postoperatively
Role of Conservative Treatment
Conservative management may be preferred when:
- Soft tissue condition is poor
- Severe medical comorbidities exist
- Smoking or diabetes increases surgical risk
- Surgery remains unsafe despite delay
Treatment includes:
- Immobilization
- Elevation
- Gradual rehabilitation
In some patients, conservative treatment provides the safest overall outcome.
Key Examination Pearls
- Tongue type and tuberosity avulsion fractures are surgical emergencies because of the risk of skin necrosis.
- Always assess soft tissue condition before definitive fixation.
- The wrinkle test is the most useful indicator of readiness for surgery.
- Extended lateral approaches carry the highest wound complication rates.
- Sinus tarsi approaches reduce soft tissue complications.
- Foot compartment syndrome may occur in up to 10% of severe calcaneal fractures.
- Open calcaneal fractures have high rates of infection and amputation.
- In calcaneal fractures, successful treatment depends as much on soft tissue management as on fracture reduction.
Leave a Reply