Courtesy: Lourenco Peixoto, Riode Janeiro, Brazil
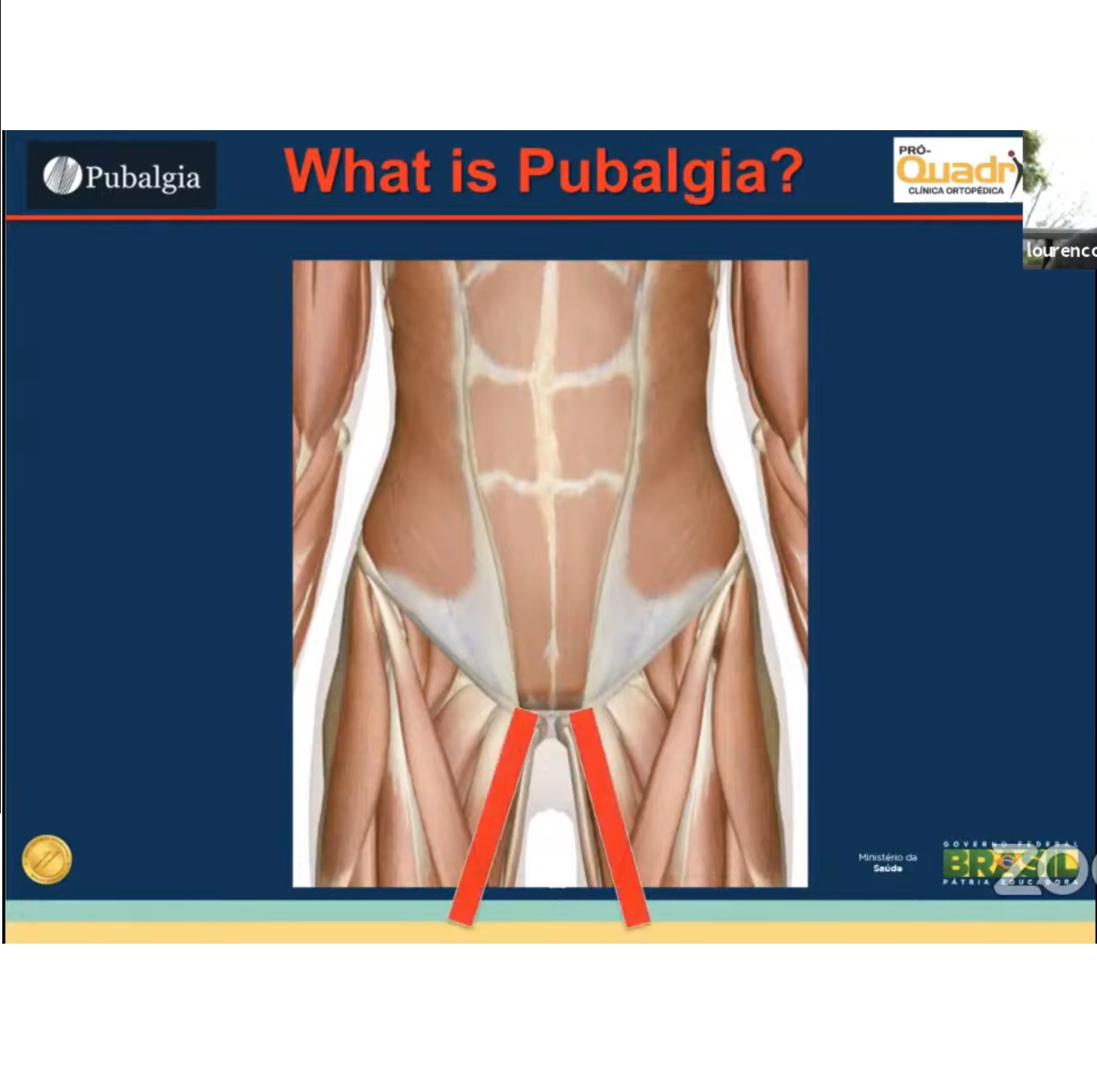
Pubalgia (Sports Groin Pain)
Introduction
Pubalgia, also known as sports groin pain, is a complex and often poorly defined cause of chronic groin pain in athletes.
It is not a single disease entity, but rather a spectrum of disorders involving:
- Muscles
- Tendons
- Pubic symphysis
- Hip joint
- Inguinal region
The condition is particularly challenging because multiple pathologies may coexist in the same athlete.
Epidemiology
Pubalgia is commonly seen in athletes involved in:
- Football (soccer)
- Running
- Hockey
- Pivoting sports
Incidence
- Approximately 0.5–6.2% of athletes develop groin pain per season.
- Up to 58% of football players experience groin pain during their careers.
- Pubalgia accounts for nearly 8% of all sports injuries.
Pathophysiology
Sports groin pain develops because of repetitive stress across the:
- Pubic symphysis
- Adductor complex
- Lower abdominal musculature
- Hip joint
Biomechanical imbalance, overuse, and reduced hip mobility contribute significantly to symptom development.
Classification of Pubalgia
Pubalgia can be broadly classified into several major pathological groups.
1. Sports Hernia (Athletic Pubalgia)
Definition
Sports hernia, also called:
- Athletic pubalgia
- Sportsman’s hernia
refers to weakness or tearing of the posterior inguinal wall without a true hernia.
Pathology
Common structures involved include:
- Posterior inguinal wall
- Transversalis fascia
Clinical Features
Patients commonly complain of:
- Chronic groin pain
- Pain radiating to the:
- Perineum
- Medial thigh
Pain is often aggravated by:
- Sprinting
- Twisting
- Kicking
- Sudden directional changes
Diagnosis
Diagnosis is based on:
- Local tenderness
- Pain reproduced during resisted movements
- Dynamic ultrasound
- MRI evaluation
Treatment
Conservative treatment may include:
- Rest
- Physiotherapy
- Core strengthening
Persistent cases often require:
- Surgical posterior wall repair
Outcomes
Surgical treatment produces excellent outcomes, with:
- Approximately 95–98% return to sport
2. Adductor Longus Pathology
Types of Injury
Adductor-related pubalgia may present as:
- Tendinopathy
- Musculotendinous injury
- Partial tear
- Complete rupture
Mechanism of Injury
A classic mechanism is:
- Sudden forceful contraction during kicking
This is commonly seen in football players.
MRI Findings
MRI may demonstrate:
- Pre-pubic aponeurosis injury
- Secondary cleft sign
Treatment
Most cases are treated conservatively with:
- Physiotherapy
- Activity modification
- NSAIDs
- Occasionally corticosteroid injections
Surgical Treatment
Resistant cases may require:
- Adductor tenotomy
3. Pubic Symphysis Pathology
Conditions Included
Pubic symphysis pathology includes:
- Osteitis pubis
- Symphyseal instability
Common Patient Groups
Frequently seen in:
- Athletes with repetitive overtraining
- Postpartum females
Clinical Features
- Local pubic tenderness
- Pain during running and cutting movements
- Pain during single-leg stance
Imaging Findings
MRI and CT may show:
- Bone marrow edema
- Symphyseal instability
- Degenerative changes
Treatment
Conservative Management
- Rest
- Physiotherapy
- Activity modification
- Injections
Surgical Treatment
Rarely required, but severe instability may require:
- Pubic symphysis arthrodesis
4. Bone Stress and Overload Injury
Pathophysiology
Repetitive overuse may produce:
- Bone marrow edema
- Stress reaction around the pubic symphysis
Treatment
Management involves:
- Load reduction
- Activity modification
- Gradual rehabilitation
5. Pubalgia Associated with Femoroacetabular Impingement (FAI)
Most Important Clinical Concept
One of the most important modern concepts in sports groin pain is the:
- Relationship between FAI and pubalgia
Hip–Pubis Relationship
Reduced hip range of motion caused by FAI increases stress on:
- Pubic symphysis
- Adductor complex
- Lower abdominal structures
This creates abnormal biomechanical loading and contributes to chronic groin pain.
Types of FAI Associated with Pubalgia
- Cam deformity
- Pincer deformity
- Mixed impingement
Clinical Insight
A very important clinical principle is:
“If pubalgia is not improving, evaluate the hip.”
Failure to recognize underlying FAI may lead to:
- Persistent symptoms
- Failed groin surgery
- Incomplete recovery
Diagnostic Approach
1. History
Important historical points include:
- Activity-related groin pain
- Sudden versus gradual onset
- Sporting activity involvement
- Aggravating movements
2. Physical Examination
Examination should include assessment for:
- Adductor tenderness
- Pubic symphysis tenderness
- Hip impingement signs
- Abdominal wall weakness
Hip examination is essential in all patients.
3. Imaging
X-Rays
Should include:
- Pelvis
- Hip views
to evaluate for:
- Cam lesions
- Pincer deformity
- Symphyseal abnormalities
MRI
MRI is useful for evaluating:
- Labral tears
- Adductor injuries
- Aponeurotic injuries
- Bone marrow edema
Dynamic Ultrasound
Especially useful for:
- Sports hernia evaluation
- Dynamic inguinal wall assessment
Treatment Principles
Conservative Management
First-line treatment typically includes:
- Rest
- Physiotherapy
- NSAIDs
- Core strengthening
- Activity modification
- Injections when indicated
Physiotherapy Goals
Rehabilitation focuses on:
- Core stability
- Hip mobility
- Adductor strengthening
- Pelvic control
Surgical Treatment
Surgery depends on the underlying pathology.
| Pathology | Surgical Treatment |
|---|---|
| Sports hernia | Posterior wall repair |
| Adductor pathology | Adductor tenotomy |
| Symphyseal instability | Arthrodesis |
| Femoroacetabular impingement | Hip arthroscopy |
Outcomes
Outcomes are generally excellent when:
- The correct pain generator is identified
- Associated hip pathology is recognized
- Treatment is individualized
More than:
- 90% of athletes return to sports
with appropriate management.
Important Clinical Pearls
- Pubalgia is a spectrum of disorders, not a single diagnosis.
- Hip pathology and groin pathology frequently coexist.
- FAI is strongly associated with sports hernia and adductor pathology.
- Failure to address underlying hip impingement may lead to persistent symptoms.
- Dynamic ultrasound is useful for sports hernia assessment.
- MRI is valuable for evaluating soft tissue and bony pathology.
- Successful treatment depends on identifying the primary pain generator.
Final Take-Home Message
Pubalgia is a complex and multifactorial cause of groin pain in athletes.
Accurate diagnosis requires:
- Careful history
- Thorough physical examination
- Appropriate imaging
- Recognition of associated hip pathology
Modern understanding emphasizes the close relationship between:
- Femoroacetabular impingement
- Adductor pathology
- Pubic symphysis overload
Comprehensive evaluation and individualized treatment provide excellent outcomes and high return-to-sport rates.
Related Posts
 Total Hip Replacement after Hip Arthroscopy
Total Hip Replacement after Hip ArthroscopyCourtesy: Leandro Alves de Oliviera, Brazil Total Hip Arthroplasty (THA) After Failed Hip Arthroscopy…
 Avoiding Complications in Hip Arthroscopy
Avoiding Complications in Hip ArthroscopyCourtesy: Thiago Busato, Hip Surgeon, Curitiba, Brazil Hip Arthroscopy: Avoiding Complications and Optimizing the…
 Cam Impingement of the Hip
Cam Impingement of the HipCourtesy: Sports Kongres, Copenhagen Prof. Siôn Glyn-Jones Chair: Prof. Per Hölmich, Dr. Olufemi Ayeni
Leave a Reply