Courtesy: Thiago Busato, Hip Surgeon, Curitiba, Brazil
Hip Arthroscopy: Avoiding Complications and Optimizing the Operative Field
Hip arthroscopy has evolved significantly over the past two decades and is now a widely accepted treatment for conditions such as femoroacetabular impingement (FAI), labral tears, and chondral injuries. As surgical techniques and instrumentation have improved, complication rates have declined substantially. Nevertheless, understanding potential complications and strategies to prevent them remains essential for achieving optimal outcomes.
Based on the uploaded article
Overview
The overall complication rate following hip arthroscopy has decreased considerably over time:
- Earlier reports: approximately 15%
- Current rates: approximately 6%
- Major complications: approximately 0.16%
Most complications are transient and improve with appropriate management. Many complications are closely related to the surgeon’s experience and learning curve.
Classification of Complications
Complications can be broadly categorized into three groups.
Avoidable Complications
These are largely technique-related and can often be prevented through careful surgical execution.
Examples include:
- Femoral head scuffing
- Labral penetration
- Inadequate correction of deformity
- Excessive correction of deformity
Minimizable Complications
These complications cannot always be completely avoided but their risk can be significantly reduced.
Examples include:
- Traction-related injuries
- Nerve injuries
- Femoral neck fractures
- Avascular necrosis (AVN)
- Adhesions
- Instrument breakage
Potential Complications
These are relatively uncommon but require vigilance and preventive measures.
Examples include:
- Infection
- Heterotopic ossification (HO)
- Fluid extravasation leading to abdominal compartment syndrome
- Venous thromboembolism (VTE)
Major Complications and Their Prevention
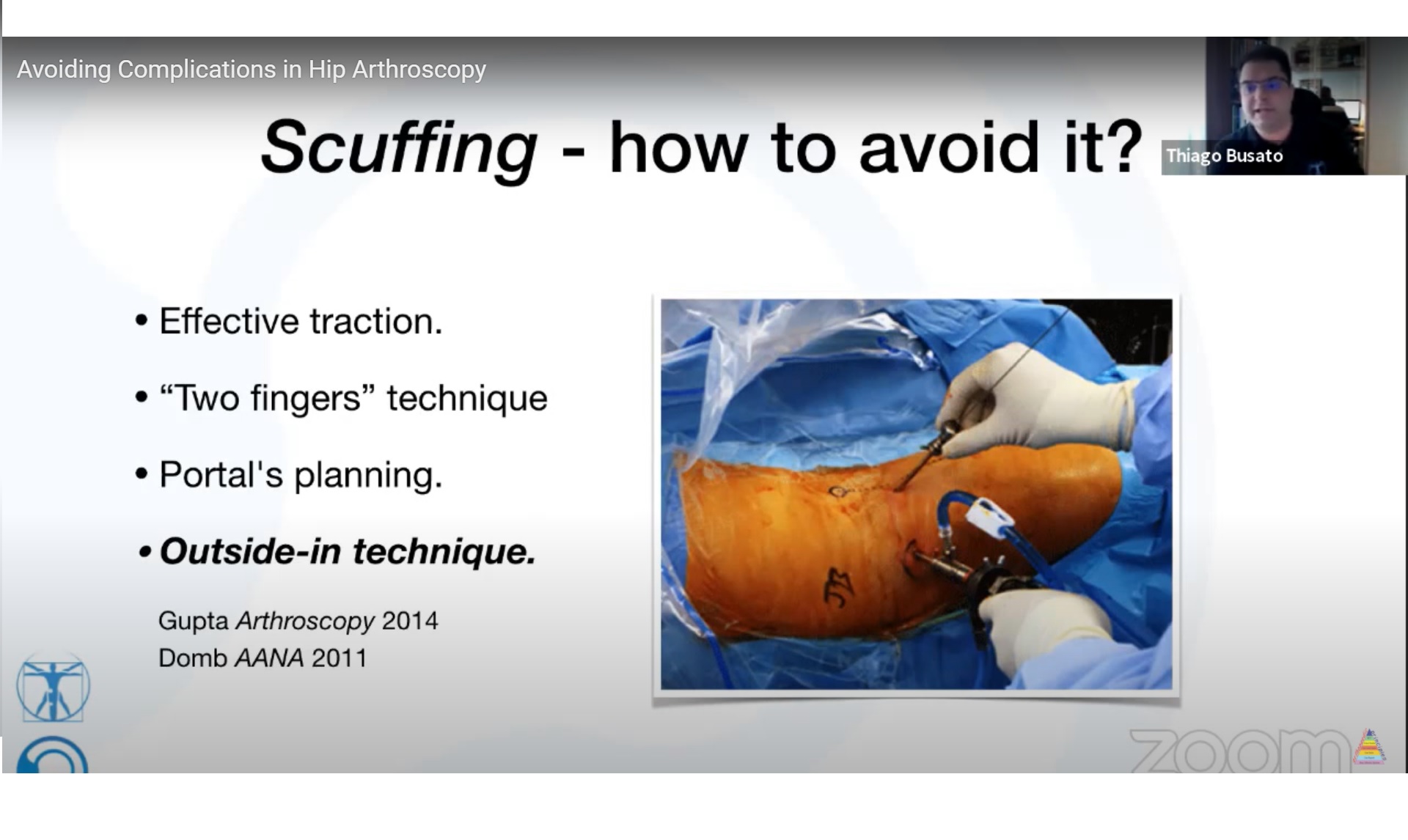
Femoral Head Scuffing
Causes
Femoral head scuffing usually occurs during difficult joint access, particularly in:
- Muscular patients
- Patients with pincer-type impingement
Prevention
- Perform an adequate traction trial before starting the procedure
- Use gentle instrumentation techniques
- Follow the “two-finger rule” to avoid excessive force
- Consider an outside-in approach when appropriate
Labral Penetration
Risk Factors
- Hypertrophic or enlarged labrum
Prevention
Safe portal entry is essential and includes:
- Air injection to confirm joint entry
- Careful control of needle bevel orientation
- Meticulous guidewire placement
Inadequate Correction
The Most Common Cause of Revision Surgery
Residual deformity accounts for the majority of revision hip arthroscopy procedures.
Common Causes
- Residual cam deformity
- Missed pathology
Prevention
Comprehensive preoperative planning is critical:
- Standard radiographs
- CT scans when indicated
- Three-dimensional planning
Intraoperative measures include:
- Fluoroscopic guidance
- Dynamic assessment of hip motion
- Identification of residual cam lesions or herniation pits
Excessive Correction
Consequences
Over-resection can result in:
- Loss of the labral suction seal
- Hip micro-instability
- Femoral neck fracture
Prevention
- Perform conservative bone resection
- Preserve labral integrity and function
- Avoid aggressive osteoplasty
Hip Instability
Causes
- Excessive bony resection
- Capsular injury
- Underlying dysplasia
Prevention
- Identify borderline dysplasia preoperatively
- Limit capsulotomy size when possible
- Perform capsular closure when indicated
- Preserve the zona orbicularis
Traction-Related Complications
Joint distraction is fundamental to hip arthroscopy but may cause complications if not carefully controlled.
Potential Problems
- Pudendal nerve neuropraxia
- Perineal soft tissue injuries
- Skin complications
Prevention
Traction Limits
- Traction time should ideally remain under two hours
- Traction force should remain below 20 kg
Patient Positioning
- Slight hip flexion
- Mild abduction
- Trendelenburg positioning when appropriate
Protection
- Use a well-padded perineal post
Nerve Injuries
The most commonly affected nerve is the lateral femoral cutaneous nerve.
Prevention
- Use blunt dissection for portal creation
- Ensure accurate portal placement
- Maintain awareness of regional anatomy throughout the procedure
Femoral Neck Fracture
Cause
Excessive cam resection weakens the femoral neck.
Prevention
- Do not remove more than 30% of the femoral neck diameter
- Avoid distal or lateral notching
- Implement protected weight-bearing for 3–4 weeks postoperatively when indicated
Avascular Necrosis
Causes
- Injury to retinacular vessels
- Excessive lateral cam resection
Prevention
- Respect known vascular safe zones
- Avoid aggressive lateral femoral neck resection
Postoperative Adhesions
Adhesions are relatively common but often remain asymptomatic.
Prevention
- Early mobilization
- Structured physiotherapy
- Continuous passive motion (CPM) when appropriate
Infection
Postoperative infection following hip arthroscopy is rare.
Prevention
- Single-dose perioperative antibiotics are generally sufficient
- Copious irrigation, often 20–30 liters of saline, helps reduce bacterial load
Heterotopic Ossification
Incidence
Reported incidence ranges from 1–6%.
Prevention
- Thorough lavage at the end of surgery
- NSAID prophylaxis, such as etoricoxib, when appropriate
Abdominal Compartment Syndrome
Although rare, this is a potentially life-threatening complication.
Causes
- Fluid extravasation
- High pump pressures
- Prolonged operative time
Clinical Signs
- Abdominal distension
- Hypotension
- Hypoxia
- Unexplained pump pressure changes
Prevention
- Maintain pump pressures below 60 mmHg
- Minimize operative time
- Monitor abdominal distension throughout the procedure
Venous Thromboembolism
Deep vein thrombosis and pulmonary embolism may be underdiagnosed after hip arthroscopy.
Prevention
- Individualized risk assessment
- Appropriate thromboprophylaxis
- Aspirin is commonly used in low- to moderate-risk patients
Patient Selection: The Most Important Factor
Appropriate patient selection remains one of the strongest predictors of successful outcomes.
Ideal Candidates
Patients with:
- Cam-type or pincer-type FAI
- Labral tears
- Joint space greater than 2 mm
- Minimal arthritic changes
Poor Candidates
Patients with:
- Advanced osteoarthritis
- Uncorrected dysplasia
- Severe deformities
- Significant torsional abnormalities
Strategies to Improve the Operative Field
Anesthetic Considerations
Many surgeons prefer:
- Combined spinal and general anesthesia
- Controlled hypotension with systolic pressures around 80–100 mmHg
Intraoperative Measures
To optimize visualization:
- Administer tranexamic acid
- Maintain pump pressure between 40–50 mmHg
- Use flow rates around 1 L/min
- Utilize smaller portals to maintain fluid seal
Preferred Surgical Workflow
A systematic approach improves efficiency and reduces complications.
Step 1
Perform pincer correction first.
Step 2
Apply traction.
Step 3
Address intra-articular pathology, including labral lesions.
Step 4
Release traction.
Step 5
Perform cam correction.
Step 6
Conduct a final dynamic assessment to ensure adequate correction and restoration of hip motion.
Learning Curve Recommendations
For surgeons early in their hip arthroscopy experience:
Suitable Early Cases
- Female patients, who often allow easier joint distraction
- Patients with straightforward anatomy
Cases to Avoid Initially
- Complex deformities
- Severe dysplasia
- Large lateral cam lesions
Stepwise Skill Development
A progressive approach is recommended:
- Portal placement
- Capsulotomy
- Osteoplasty
- Labral repair
Key Take-Home Messages
- Hip arthroscopy is a safe procedure with a relatively low complication rate when performed appropriately.
- Inadequate correction remains the leading cause of revision surgery.
- Proper patient selection is critical to achieving successful outcomes.
- Traction-related complications can be minimized through careful positioning and time limits.
- Preservation of the labrum, capsule, and vascular structures is essential.
- Thorough preoperative planning and dynamic intraoperative assessment help avoid both under-correction and over-correction.
- A structured surgical workflow and gradual progression through the learning curve can significantly reduce complications.


Leave a Reply