Courtesy: Leandro Alves de Oliviera, Brazil
Total Hip Arthroplasty (THA) After Failed Hip Arthroscopy
Introduction
Hip arthroscopy has become a widely accepted procedure for the treatment of:
- Femoroacetabular impingement (FAI)
- Labral tears
- Chondral lesions
- Loose bodies
- Ligamentum teres pathology
- Snapping hip syndrome
Although hip arthroscopy is an important hip preservation procedure, some patients eventually progress to:
- Total Hip Arthroplasty (THA)
Conversion to THA is generally considered:
- Failure of hip preservation surgery
Understanding which patients are likely to fail arthroscopy is critical for appropriate patient selection and surgical planning.
Common Indications for Hip Arthroscopy
Hip arthroscopy is commonly performed for:
- Femoroacetabular impingement (most common indication)
- Labral tears
- Chondral defects
- Loose bodies
- Ligamentum teres injuries
- Snapping hip disorders
The Most Important Clinical Question
When Should Arthroscopy Be Avoided?
A key principle in hip preservation surgery is recognizing:
- Which patients are poor candidates for arthroscopy
In certain situations, patients may achieve better outcomes with:
- Primary Total Hip Arthroplasty
rather than undergoing unsuccessful hip preservation procedures.
Poor Candidates for Hip Arthroscopy
Absolute and Relative Contraindications
Patients with the following features have poorer outcomes after arthroscopy:
- Joint space less than 2 mm
- Established osteoarthritis
- Tönnis grade 2 or higher
- Severe cartilage damage
- Femoral head chondral lesions
- Dysplasia without corrective surgery
- Advanced age with cartilage degeneration
- Significant degenerative changes
Advanced Age
Patients older than:
- 40 years
particularly with cartilage damage, have an increased risk of failure after arthroscopy.
Why These Patients Fail
These patients often already have:
- Irreversible joint degeneration
As a result:
- Arthroscopy cannot adequately restore hip mechanics
and progression to THA becomes likely.
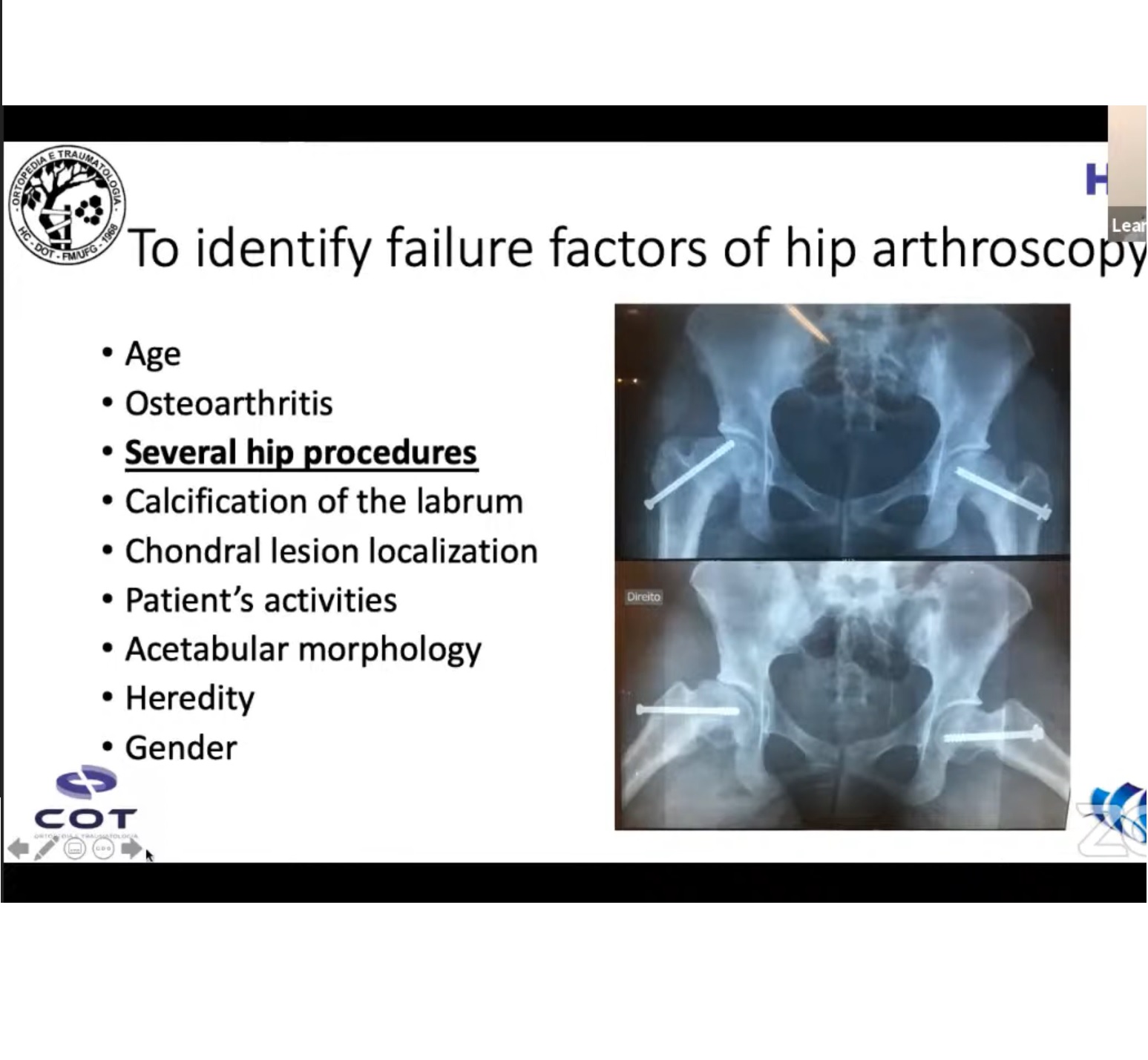
Causes of Failure of Hip Arthroscopy
Failure can be divided into:
- Patient-related factors
- Surgical factors
Patient-Related Factors
Important patient-related risk factors include:
- Age greater than 40 years
- Osteoarthritis
- Severe cartilage damage
- Dysplasia
- Coxa profunda
- Protrusio acetabuli
- Obesity
- Genetic predisposition
- High-demand athletic activity
Cartilage Damage
Severe cartilage injury is one of the strongest predictors of failure.
Outerbridge Classification of Cartilage Damage
| Grade | Description |
|---|---|
| I | Cartilage softening |
| II | Fragmentation less than 1.5 cm |
| III | Fragmentation greater than 1.5 cm |
| IV | Exposed subchondral bone |
Grades III and IV are associated with:
- Poor prognosis after arthroscopy
Surgical Factors Leading to Failure
1. Inadequate Cam Resection
The most common technical error is:
- Under-resection of the cam deformity
Residual impingement continues to damage:
- Labrum
- Cartilage
leading to persistent symptoms.
2. Poor Labral Management
Historically, labral debridement was common.
Current evidence supports:
- Labral preservation
- Labral repair
- Labral reconstruction when necessary
Debridement alone is associated with:
- Inferior long-term outcomes
3. Inadequate Capsular Management
Failure to preserve or repair the capsule may result in:
- Instability
- Persistent pain
4. Missed Pathology
Failure to recognize associated conditions such as:
- Dysplasia
- Version abnormalities
- Chondral injury
may contribute to poor outcomes.
Risk of Conversion to THA
Failure Rates
Reported failure rates after hip arthroscopy are approximately:
- 16% within 2 years
Conversion Rates
Conversion to THA occurs in approximately:
- 7–20% of patients
depending on patient selection and degree of degeneration.
Time to Conversion
The average time from arthroscopy to THA is approximately:
- 23–29 months
Predictors of Conversion to THA
Several factors increase the likelihood of requiring THA after arthroscopy.
Major Predictors
- Increasing age
- Poor preoperative hip scores
- Severe cartilage damage
- Joint space narrowing
- High alpha angle
- Femoral version abnormalities
- Osteoarthritis
Joint Space Narrowing
Joint space less than:
- 2 mm
is one of the strongest predictors of poor outcome and early THA conversion.
Outcomes of THA After Previous Hip Arthroscopy
Compared with primary THA, conversion THA after arthroscopy is generally associated with:
- Greater technical difficulty
- Higher complication rates
- Slightly inferior functional outcomes
Comparison: THA After Arthroscopy vs Primary THA
| Parameter | THA After Arthroscopy | Primary THA |
|---|---|---|
| Surgical time | Longer | Shorter |
| Infection risk | Higher | Lower |
| Dislocation risk | Higher | Lower |
| Functional outcome | Slightly worse | Better |
Why Conversion THA Is More Difficult
Prior arthroscopy may create:
- Scar tissue
- Capsular changes
- Altered anatomy
These factors increase surgical complexity during THA.
Complications
Potential complications after THA following arthroscopy include:
- Infection
- Dislocation
- Persistent stiffness
- Technical challenges during exposure
Clinical Pearls
1. Proper Patient Selection Is the Most Important Factor
A key principle is:
“The success of hip arthroscopy depends more on indication than technique.”
2. Avoid Arthroscopy in Advanced Arthritis
Hip arthroscopy should generally be avoided when patients have:
- Advanced osteoarthritis
- Severe cartilage loss
- Joint space less than 2 mm
These patients often benefit more from:
- Early Total Hip Arthroplasty
3. Technical Precision Is Essential
Successful arthroscopy requires:
- Adequate cam resection
- Labral preservation and repair
- Proper capsular management
4. Type of FAI Influences Outcome
Patients with isolated:
- Cam deformities
generally have better outcomes than patients with:
- Pincer deformity
- Combined impingement
Important Case-Based Insight
Patients with:
- Severe cartilage degeneration
- Soft femoral head cartilage
- Advanced chondral lesions
may progress rapidly toward:
- End-stage arthritis
- Early THA
despite arthroscopic intervention.
Key Take-Home Messages
- Hip arthroscopy is an effective hip preservation procedure when performed in properly selected patients.
- Advanced arthritis and severe cartilage damage are major predictors of failure.
- Joint space less than 2 mm strongly predicts conversion to THA.
- Under-resection of cam lesions is the most common technical cause of failure.
- Labral repair is preferred over debridement.
- Conversion THA after arthroscopy is technically more challenging than primary THA.
- Appropriate patient selection is more important than surgical technique alone.
Final Take-Home Message
The primary goal of hip arthroscopy is:
- Preservation of the native hip joint
However, not all patients are ideal candidates for hip preservation surgery.
Recognizing patients with:
- Advanced degeneration
- Significant cartilage loss
- Established osteoarthritis
is critical to avoid failed procedures and delayed definitive treatment.
In appropriately selected patients, early Total Hip Arthroplasty may provide:
- Better pain relief
- Faster recovery
- More predictable outcomes
than unsuccessful hip preservation attempts.
Leave a Reply