Courtesy: Prof Robert Ashford, President, British Orthopaedic Oncology Society
Principles of Treating Soft Tissue Sarcomas
Overview
Soft tissue sarcomas are rare malignant tumors arising from mesenchymal tissues such as:
- Muscle
- Fat
- Fibrous tissue
- Blood vessels
- Peripheral nerves
They are biologically heterogeneous tumors with varying:
- Aggressiveness
- Local recurrence risk
- Metastatic potential
- Response to treatment
Most patients present with a painless soft tissue mass.
Epidemiology
- Sarcomas account for approximately 1.4% of all new cancers
- About 90% arise from soft tissues
- Incidence: approximately 20–30 cases per million annually
- Overall 5-year survival: around 55%
- Can occur at any age and at any anatomical site
Clinical Features Suggesting Malignancy
Features raising suspicion for sarcoma include:
- Size >5 cm
- Deep location beneath fascia
- Rapid increase in size
- Painful mass
- Recurrence after previous excision
- Calcification or bone erosion on X-ray
- Change in size over time
Most sarcomas initially present as a painless lump mistaken for benign lesions such as:
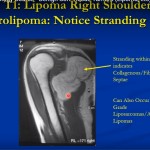
- Lipoma
- Hematoma
Classification
Soft tissue sarcomas are classified based on:
- Histological subtype
- Tumor differentiation
- Molecular characteristics
More than 100 histological subtypes exist.
Common examples:
- Undifferentiated pleomorphic sarcoma
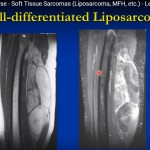
- Liposarcoma
- Synovial sarcoma
- Rhabdomyosarcoma
Etiology and Risk Factors
Recognized risk factors include:
Environmental
- Prior radiation exposure
- Certain chemical exposures
Genetic Syndromes
- Neurofibromatosis
- Li–Fraumeni syndrome
- Hereditary retinoblastoma
Viral Associations
Particularly in immunocompromised patients:
- Epstein–Barr virus
- Human herpesvirus 8
There is no strong evidence linking:
- Trauma
- Orthopedic implants
to sarcoma development.
Imaging Evaluation
1. Ultrasound
- Often initial investigation
- Operator dependent
2. MRI (Most Important)
MRI is the imaging modality of choice for extremity soft tissue sarcomas.
Advantages:
- Defines local extent
- Evaluates neurovascular involvement
- Assesses compartment involvement
- Helps biopsy planning
3. CT Scan
Useful for:
- Retroperitoneal sarcomas
- Metastatic staging
- Pulmonary metastasis detection
4. PET-CT
May help in:
- Detecting recurrence
- Guiding biopsy
- Assessing metastatic disease
Biopsy Principles
Golden Rule
Biopsy should be carefully planned because poorly placed biopsy tracts can compromise future limb-sparing surgery.
Preferred Method
Core Needle Biopsy
- Image-guided
- Standard technique
- Minimally invasive
Excision Biopsy
May be considered only for:
- Small
- Superficial lesions
Open Biopsy Principles
- Longitudinal incision
- Minimal tissue contamination
- Avoid neurovascular injury
- Include tumor-normal tissue interface
Frozen section is mainly used to confirm:
- Adequate tissue sampling
rather than establish final diagnosis.
Staging and Grading
Staging is based on:
- Tumor size
- Nodal involvement
- Metastasis
Important concepts:
- Larger tumors have worse prognosis
- Approximately one-third are low-grade
- Remaining tumors are high-grade
Prognostic Factors
Poor prognostic indicators include:
- Metastasis at presentation
- Large tumor size
- Deep location
- Older age
- Positive surgical margins
- Elevated inflammatory markers
Multidisciplinary Management
Management requires coordination among:
- Orthopedic oncologists
- Radiologists
- Pathologists
- Medical oncologists
- Radiation oncologists
- Plastic surgeons
- Specialist nurses
Treatment plans should distinguish:
- Curative intent
- Palliative intent
Surgical Management
Most Important Treatment
Surgery remains the most effective curative treatment.
Limb Salvage
Preferred whenever feasible.
Amputation is now uncommon.
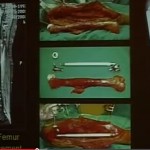
Surgical Principles
- Achieve wide excision margins
- Avoid tumor contamination
- Preserve limb function where possible
- Plan reconstruction carefully
Most procedures involve:
- Wide local excision
rather than radical compartmental resections.
Surgical Margins
Adequate margins are essential for:
- Local control
- Reduced recurrence risk
Important concept:
- Planned positive margins are preferable to unplanned incomplete excisions.
Reconstruction
Large resections may require:
- Skin grafts
- Muscle flaps
- Free tissue transfer
Plastic surgical collaboration is often necessary.
Radiotherapy
Radiotherapy may be used:
- Preoperatively
- Postoperatively
- Occasionally as primary treatment
Preoperative Radiotherapy
Advantages:
- Better target definition
- Smaller radiation field
Disadvantage:
- Increased wound complications
Postoperative Radiotherapy
Advantages:
- Final pathology available before treatment
Disadvantages:
- Increased fibrosis
- Joint stiffness
- Fracture risk
Chemotherapy
Usually reserved for:
- Advanced disease
- Metastatic disease
- Specific chemosensitive subtypes
Responsive tumors include:
- Rhabdomyosarcoma
- Synovial sarcoma
Common regimens:
- Anthracycline-based chemotherapy
- Ifosfamide combinations
Metastatic Disease
Most Common Site
- Lung metastasis
Median survival after metastasis:
- Less than one year
Selected patients with isolated pulmonary metastases may benefit from:
- Pulmonary metastasectomy
Key Orthopedic Oncology Principles
- Suspect sarcoma in enlarging deep soft tissue masses
- Any mass >5 cm requires careful evaluation
- MRI before biopsy whenever possible
- Biopsy must follow oncologic principles
- Surgery with adequate margins is critical
- Multidisciplinary care improves outcomes
- Long-term follow-up is essential for recurrence detection
Leave a Reply