EPIDEMIOLOGY
-
Physeal injuries account for approximately 21 percent of all paediatric fractures (average of six large series).
Distribution by Location
-
Phalanges: 37 percent
-
Distal radius: 18 percent
-
Distal tibia: 11 percent
-
Distal fibula: 7 percent
-
Metacarpals: 6 percent
-
Distal femur: uncommon but high risk for growth arrest
WHY PHYSEAL INJURIES OCCUR
Key contributing factors include:
-
Tension forces across the physis
-
Weakening of the perichondral ring, especially toward the end of growth
-
Increasing skeletal mass, with increasing kinetic energy during trauma
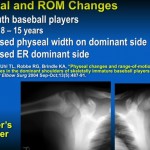
UNIQUE FEATURES OF THE DISTAL FEMORAL PHYSIS
-
The distal femoral physis is subjected predominantly to shear forces.
-
These forces directly affect the reproducing cells of the growth plate.
-
Consequently, injuries at this site have a high rate of growth arrest, even with minimal displacement.
SITE OF PHYSEAL FAILURE
-
The physis most commonly fails at the zone of hypertrophy.
PATHOLOGY OF PHYSEAL ARREST
-
Growth arrest occurs due to formation of a physeal bar or bony bridge.
-
The physeal bar is composed of dense cortical bone.
-
Tension forces from adjacent functioning physis stimulate cortical bone formation.
-
On radiographs, the bar appears sclerotic.
PATTERNS OF PHYSEAL ARREST
Classification Systems
-
Ogden classification (A, B, C)
-
Bright classification (C, B, A)
-
Peterson descriptive classification (most practical and clinically useful)
Peterson Classification of Physeal Arrest
Central Physeal Bar
-
Central growth arrest
-
Peripheral physis remains intact
-
Produces the volcano effect
Peripheral Physeal Bar
-
Involves the edge of the physis
-
Leads to progressive angular deformity
Linear (Longitudinal) Physeal Bar
-
Vertical bar extending from one cortex to the opposite cortex
-
Commonly associated with Salter–Harris type IV injuries
-
Results in angulation and limb shortening
RADIOGRAPHIC FEATURES ON PLAIN RADIOGRAPHS
-
Physeal narrowing
-
Areas of sclerotic bone
-
Absence of Harris growth arrest line migration
-
Progressive angular deformity
-
Limb length discrepancy
IMAGING INVESTIGATIONS
Computed Tomography
-
Helpful for precise localization and size measurement of the physeal bar
-
Allows three-dimensional assessment
Magnetic Resonance Imaging
-
Gold standard investigation
-
Physeal bar appears dark because it lacks water content
-
Clearly differentiates bone, cartilage, and remaining physis
-
Essential for surgical planning
IMPORTANCE OF LOCALIZATION OF THE PHYSEAL BAR
The location of the bar determines:
-
Type of deformity
-
Surgical approach
-
Probability of successful resection
LOCATION AND RESULTING DEFORMITY
-
Central bar: symmetrical growth disturbance, volcano effect
-
Peripheral bar: severe angular deformity
-
Linear bar: combined angulation and shortening
LOCATION AND SUCCESS OF RESECTION
-
Central bar: symmetrical growth, good success rate
-
Peripheral bar: asymmetrical growth, poor success rate
FACTORS AFFECTING SUCCESS OF BAR RESECTION
-
Size of the bar: less than 30 percent of physeal area is favorable
-
Age: younger patients with more than 2 years of growth remaining
-
Duration since injury: more than 2 years reduces success
-
Etiology:
-
Trauma: better prognosis
-
Tumor, infection, irradiation: poor prognosis
-
IDEAL CANDIDATE FOR PHYSEAL BAR RESECTION
-
Young patient
-
Small physeal bar
-
Traumatic etiology
-
Recent onset
-
Central or linear bar
POOR CANDIDATE FOR RESECTION
-
Older patient
-
Large physeal bar
-
Infection or radiation-related etiology
-
Peripheral physeal bar
SURGICAL APPROACH BASED ON BAR LOCATION
-
Central bar: large metaphyseal window
-
Peripheral bar: direct approach to the bar
-
Linear bar: cortical-to-cortical osseous tunnel through a large metaphyseal window
Key principle:
-
Surgical approach must be perpendicular to the physis
INTERPOSITION MATERIALS AFTER BAR RESECTION
-
Autogenous fat graft
-
Cranioplast (methyl methacrylate without barium)
-
Silastic sheets (historical use, no longer available in some regions)
ALTERNATIVES TO PHYSEAL BAR RESECTION
-
Physeal distraction
-
Used when resection is not feasible or prognosis is poor
REQUIREMENTS FOR GOOD OUTCOMES
-
Detailed knowledge of physeal anatomy
-
Understanding patterns of physeal arrest
-
Proper case selection
-
Accurate preoperative planning
-
Meticulous surgical technique
-
Awareness of alternatives to resection
-
Long-term follow-up to detect recurrence early
KEY TAKEAWAY
Successful management of physeal injuries depends not only on treating the initial fracture but also on early recognition, precise imaging, correct classification, and appropriate intervention to prevent or manage growth arrest.


Leave a Reply