Courtesy: Prof Nabil Ebraheim, University of Toledo, Ohio, USA
Pediatric Elbow X-ray Interpretation – Stepwise Approach
Why This Topic Is Important
- Many pediatric elbow fractures are occult and may not be obvious on initial X-rays
- A normal-looking X-ray does not exclude fracture
- Missed injuries can result in:
- Malunion
- Deformity
- Loss of motion
- Long-term disability
Step 1: Ensure Proper X-ray Quality
Essential Views
- Proper AP view
- True lateral view
Important Lateral View Feature
- A proper lateral X-ray should demonstrate the:
- Figure-of-8 appearance
- Hourglass appearance
If absent:
- Repeat the X-ray before interpretation
Step 2: Identify Ossification Centers (CRITOE)
Elbow ossification centers CRITOE
| Letter | Ossification Center | Approximate Age |
|---|---|---|
| C | Capitellum | 1 year |
| R | Radial head | 3 years |
| I | Medial epicondyle | 5 years |
| T | Trochlea | 7 years |
| O | Olecranon | 9 years |
| E | Lateral epicondyle | 11 years |
Key Clinical Points
- Always correlate ossification centers with patient age
- Missing or displaced ossification center suggests fracture
- Carefully inspect for:
- Medial epicondyle incarceration inside the joint
Step 3: Examine Bone Carefully
Look For
- Cortical disruption
- Subtle angulation
- Irregular bone contour
- Small avulsion fragments
Commonly Missed Fracture Sites
- Supracondylar fracture of humerus
- Lateral condyle fracture of humerus
- Radial neck fracture
- Olecranon fractures
Step 4: Fat Pad Sign – Clue to Occult Fracture
Normal Fat Pads
| Fat Pad | Normal Appearance |
|---|---|
| Anterior fat pad | May be visible |
| Posterior fat pad | Normally not visible |
Abnormal Findings
Sail Sign
- Elevated triangular anterior fat pad
Posterior Fat Pad
- Always abnormal if visible
Clinical Significance
Suggests occult fracture even if fracture line is not seen.
Most common associated injuries:
- Supracondylar fracture of humerus
- Radial neck fracture
- Lateral condyle fracture
Step 5: Alignment Lines – Very Important
1. Anterior Humeral Line
Technique
- Draw a line along the anterior cortex of the humerus on lateral view
Normal
- Passes through the middle third of the capitellum
Abnormal
- Failure to intersect middle third suggests:
- Extension-type supracondylar fracture
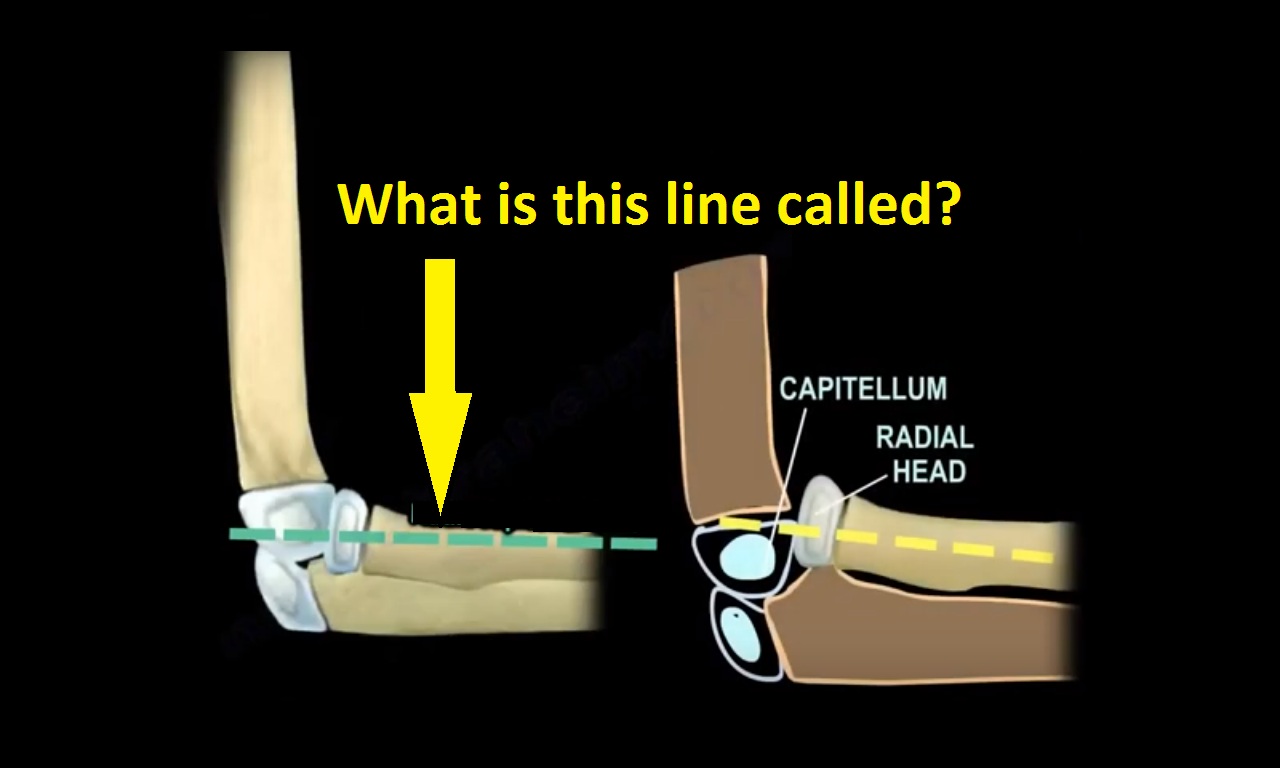
2. Radiocapitellar Line
Technique
- Draw a line along the radial neck
Rule
- Must intersect the capitellum in all views
If Abnormal, Consider
- Radial head dislocation
- Monteggia fracture-dislocation
Important Tip
- Radial neck line is more accurate than radial shaft line in children
Step 6: Use the Capitellum as the Landmark
The capitellum is:
- The first elbow ossification center to appear
- A critical reference point in pediatric elbow imaging
Clinical Use
Helps identify:
- Elbow dislocation
- Monteggia injuries
- Alignment abnormalities
- Transphyseal distal humerus injuries
Important Special Diagnostic Situations
Monteggia Injury
Monteggia fracture-dislocation
Features
- Ulna fracture or plastic deformation
- Radial head dislocation
Diagnosis
- Best detected using radiocapitellar alignment
Transphyseal Separation of Distal Humerus
Seen In
- Infants and very young children
Mimics
- Elbow dislocation
Differentiating Features
| Feature | Elbow Dislocation | Transphyseal Separation |
|---|---|---|
| Radiocapitellar line | Disrupted | Maintained |
| Olecranon displacement | Posterolateral | Posteromedial |
Practical Interpretation Sequence
- Confirm adequate X-ray quality
- Identify CRITOE ossification centers
- Examine cortex carefully
- Assess fat pads
- Draw:
- Anterior humeral line
- Radiocapitellar line
- Use capitellum as reference landmark
- Form differential diagnosis
High-Yield Exam Pearls
- Posterior fat pad indicates occult fracture until proven otherwise
- CRITOE sequence must be memorized
- Anterior humeral line assesses supracondylar fracture alignment
- Radiocapitellar line evaluates radial head alignment
- Never interpret a poor-quality lateral X-ray
- Missing medial epicondyle after elbow dislocation suggests incarcerated fragment

Leave a Reply