Courtesy: Amr Abdelgawad, Maimonaides Medical Centre, NY, USA
Apophyseal and Avulsion Injuries
Apophysis
- Secondary ossification center located outside the joint where tendons attach.
Common apophyseal attachments
- Calcaneus: Achilles tendon.
- Tibial tubercle: Patellar tendon.
- Anterior inferior iliac spine (AIIS): Rectus femoris.
- Anterior superior iliac spine (ASIS): Sartorius.
- Ischial tuberosity: Hamstrings.
- Iliac crest: Abdominal muscles.
Treatment
- Rest.
- Activity restriction.
- Most injuries are managed nonoperatively.
Pediatric Hip Dislocation
Features
- Usually posterior dislocation.
- Limb is adducted and internally rotated.
Management
- Gentle reduction under anesthesia.
- Avoid physeal separation.
- Open reduction for irreducible or nonconcentric reductions.
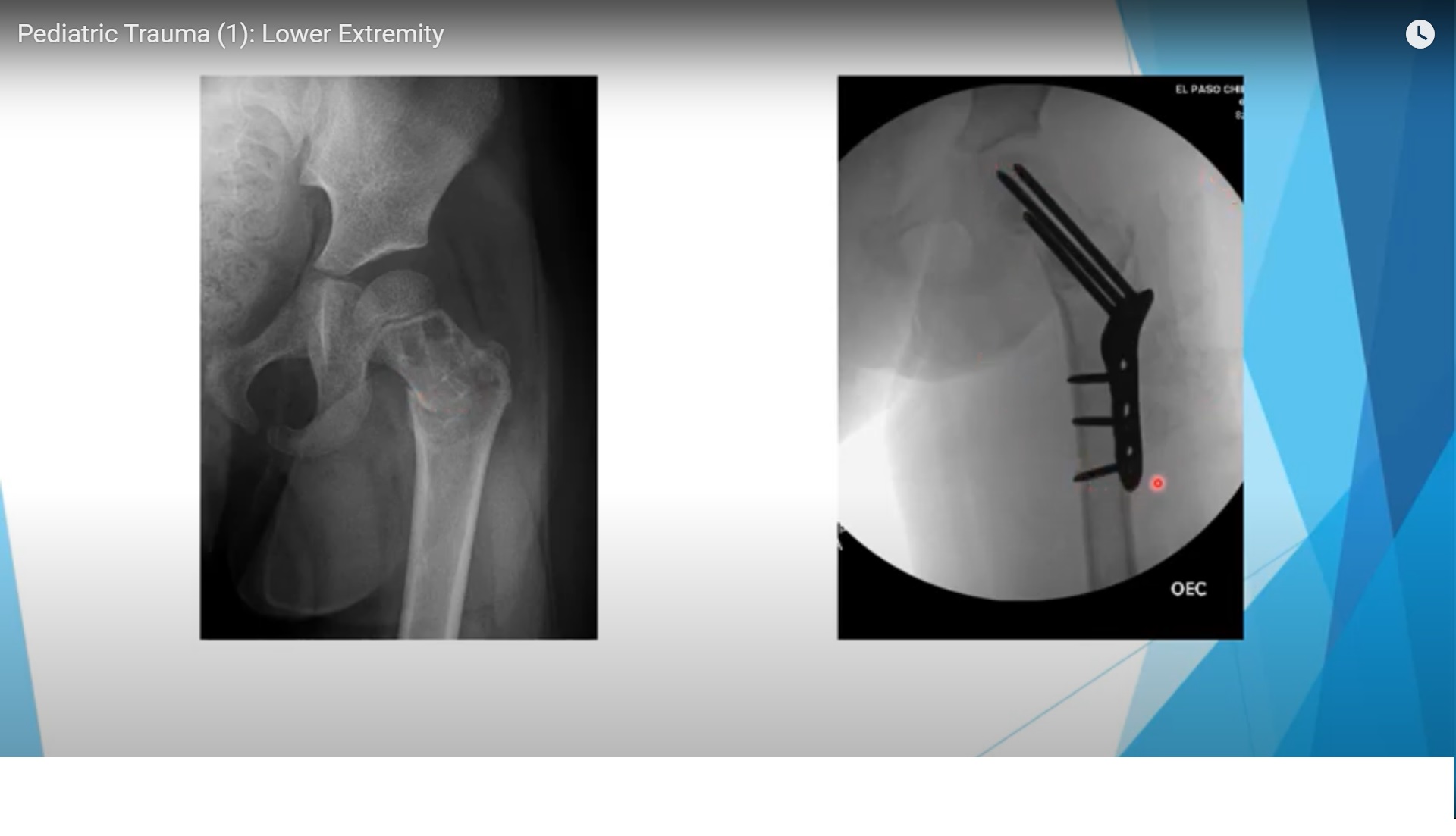
Proximal Femur Fractures
Delbet Classification
Type I: Transphyseal
- Highest risk of avascular necrosis.
Type II: Transcervical
- High risk of avascular necrosis.
Type III: Cervicotrochanteric
- Moderate risk of avascular necrosis.
Type IV: Intertrochanteric
- Lowest risk of avascular necrosis.
Complications
- Avascular necrosis.
- Nonunion.
- Varus collapse.
Treatment
- Emergency fixation.
- Capsulotomy or aspiration to reduce intracapsular pressure.
- Fixation with screws, pins with hip spica, or pediatric hip plates.
Femoral Shaft Fractures
Age based treatment
Less than 6 months
- Pavlik harness.
6 months to 5 years
- Immediate hip spica cast.
5 to 12 years
- Transverse fractures: Flexible intramedullary nails.
- Comminuted fractures: Submuscular plating.
More than 12 years or weight more than 45 kg
- Rigid intramedullary nail using a lateral entry point.
Flexible Intramedullary Nails
Best indications
- Midshaft fracture.
- Transverse pattern.
- Noncomminuted fracture.
- Weight less than 45 kg.
Key point
- Correct nail diameter is essential.
Most common complication
- Knee irritation.
Rigid Intramedullary Nailing
Important principle
- Use lateral trochanteric entry.
- Avoid piriformis entry because of the risk of avascular necrosis.
External Fixation
Indications
- Open fractures.
- Polytrauma.
Complication
- Refracture after removal.
Submuscular Plating
Indications
- Comminuted fractures.
- Proximal or distal femoral shaft fractures.
Advantages
- Preserves alignment.
- Maintains limb length.
Nonaccidental Trauma
Clinical clues
- Femur fracture in a nonambulatory child.
- Multiple fractures.
- Delayed presentation.
- Inconsistent history.
Important point
- Spiral fracture alone does not indicate child abuse.
Management
- Notify child protection services when abuse is suspected.
Distal Femoral Physeal Injuries
Features
- Highest risk of growth arrest.
- Mammillary interdigitation contributes to physeal injury.
Complications
- Limb length discrepancy.
- Angular deformity.
Management
- Urgent reduction.
- Screw fixation for large metaphyseal fragments.
- Kirschner wires for smaller fragments.
Patellar Sleeve Fracture
Features
- Small bony fragment with a large cartilaginous component.
- Disruption of the extensor mechanism.
Treatment
- Open reduction and internal fixation.
Tibial Spine (Eminence) Fracture
Equivalent injury
- Anterior cruciate ligament avulsion.
Classification
Type I
- Nondisplaced.
Type II
- Hinged displacement.
Type III
- Completely displaced.
Special point
- Irreducible Type III fractures often have entrapment of the anterior horn of the medial meniscus.
Treatment
- Type I: Cast immobilization.
- Type II: Closed reduction.
- Type III: Surgical fixation.
Tibial Tubercle Avulsion
Mechanism
- Common in adolescents during jumping activities.
Complication
- Compartment syndrome due to injury of the recurrent anterior tibial artery.
Treatment
- Open reduction and screw fixation.
Proximal Tibial Metaphyseal Fracture
Complication
- Cozen phenomenon causing progressive valgus deformity.
Treatment
- Observation.
- Guided growth if deformity persists.
Toddler Fracture
Features
- Spiral fracture of the tibial shaft.
- Usually occurs in children aged 2 to 3 years.
- Fibula remains intact.
- Initial radiographs may be normal.
Treatment
- Above knee cast.
Tibial Shaft Fracture
Treatment
- Usually managed conservatively.
Important consideration
- Monitor closely for compartment syndrome.
Distal Tibial Physeal Injuries
Complication
- Growth arrest in up to 50 percent of cases.
Management
- Salter Harris Type I and II: Closed reduction.
- Salter Harris Type III and IV: Open reduction and internal fixation.
Special Fractures
Tillaux Fracture
- Avulsion fracture of the anterolateral distal tibial epiphysis.
- Caused by the anterior inferior tibiofibular ligament.
- Treated with open reduction and internal fixation.
Triplane Fracture
- Fracture involving three anatomical planes.
- Requires anatomical articular reduction and open reduction with internal fixation.
Pediatric Foot Fractures
Most common fracture
- Base of the first metatarsal.
Exam Pearls
- Femur fracture in a nonambulatory child should raise suspicion of child abuse.
- Flexible intramedullary nails are best for transverse midshaft femoral fractures.
- The most common complication of flexible nails is knee irritation.
- Distal femoral physeal injuries carry the highest risk of growth arrest.
- Irreducible Type III tibial spine fractures are commonly associated with meniscal entrapment.
- Tibial tubercle avulsion fractures are associated with compartment syndrome.
- Proximal tibial metaphyseal fractures may lead to Cozen valgus deformity.
Leave a Reply