Courtesy: CR Chandrasekhar, Consulant Orthopaedic Surgeon Liverpool
Alpesh Mistry, MSK Radiologist, Liverpool
Susha Varghese, Pathologist, Liverpool
Practical Guide to Diagnosing Soft Tissue Masses
Overview
- Purpose: Concise, practical guidance on identifying and diagnosing soft tissue masses for clinicians.
- Audience: General surgeons, orthopedic surgeons, radiologists, pathologists, and other clinicians who evaluate soft tissue lumps.
- Main themes: clinical assessment, imaging strategy, biopsy technique, pathology role, multidisciplinary care.
Definitions and Key Differences
- Tumor: an abnormal mass of tissue in which cells continue to grow or fail to die normally; commonly described by patients as a lump, bump, or swelling.
- Benign tumor: usually localized, often encapsulated, slow growing, and unlikely to invade neighboring tissues or metastasize.
- Malignant tumor: has the capacity to invade locally and to spread to distant sites; metastasis is the defining feature of malignancy.
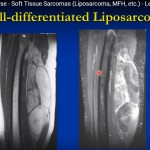
- Soft tissue sarcoma: a malignant tumor arising from connective tissue, uncommon, and often diagnosed at a larger size than common epithelial cancers.
Clinical Assessment
- History: obtain a clear timeline for the lump, associated symptoms (pain, growth), prior trauma, anticoagulant use, and relevant past or family medical history.
- Examination: inspect, palpate and assess mobility, consistency, tenderness, relation to skin, and whether the lump is superficial or deep relative to the deep fascia.
- Formulate a working diagnosis (benign, malignant, or indeterminate) based on history and examination before ordering investigations.
- Treat the patient, not just the lesion: consider comorbidities, social circumstances, and whether local resources can safely manage the case; refer when appropriate.
Common Benign Lesions
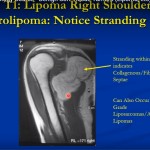
- Lipoma: common, soft, lobulated, mobile, usually non-tender; may occur in many locations.
- Ganglion cyst: typical around the wrist, hand, or foot; cystic and often compressible.
- Bursa enlargement (bursitis): frequently at predictable locations such as prepatellar and olecranon bursa.
- Epidermal inclusion cyst: contains keratinous debris and may be tethered to the skin.
- Vascular malformations and hemangiomas, fibromas, schwannomas and chronic hematoma (especially in patients on anticoagulants).
- Infective or inflammatory masses can mimic tumors and often improve with appropriate treatment.
Red Flags Suggesting Possible Sarcoma
- Size greater than 5 cm.
- Increasing size or rapid growth.
- Deep to the deep fascia (subfascial).
- New, unexplained lump without a convincing benign explanation.
- Recurrent lump after prior excision.
- Painful lump (though some sarcomas may be painless).
Imaging Strategy
- Use imaging to characterize the lesion, guide management, and plan biopsy or surgery.
- Ultrasound: first-line triage for many superficial lumps; operator dependent, rapid, low-cost, and provides dynamic assessment and vascularity via Doppler.
- Magnetic resonance imaging: used for indeterminate or suspicious lesions, lesions deep to fascia, or when local staging and surgical planning are required; typical protocol includes T1-weighted and fluid-sensitive sequences with fat suppression and axial planes.
- Computed tomography: reserved for limited indications, such as evaluation of mineralization, bone involvement, or when magnetic resonance imaging is contraindicated.
- Radiographs (plain X-rays): helpful when calcification or bony change is suspected.
- Imaging limitations: benign and malignant lesions can overlap in appearance; correlate with clinical information.
Role of the Radiologist and Biopsy Guidance
- Radiologists help triage lesions (benign, indeterminate, or suspicious) and select the most appropriate imaging modality.
- Ultrasound is frequently used to guide percutaneous core needle biopsy for accessible lesions.
- Computed tomography guidance is used for deep, retroperitoneal, or anatomically difficult targets where ultrasound visualization is inadequate.
- Magnetic resonance imaging guided biopsy is possible but requires specialized setup and is less commonly used because of logistical complexity.
- Biopsy planning must be coordinated with the surgeon to ensure the biopsy tract lies within the eventual surgical field to avoid contaminating otherwise uninvolved compartments.
Biopsy Technique and Diagnostic Yield
- Image-guided percutaneous core needle biopsy is the preferred initial approach when imaging or clinical features are not convincingly benign.
- Core needle biopsy typically aims to obtain 3–5 cores with 14 gauge preferred when feasible; smaller gauge needles may be used for very firm lesions.
- Diagnostic accuracy of image-guided core needle biopsy is high when representative tissue is obtained; sampling error occurs with necrotic or heterogeneous tumors.
- Small, superficial lesions less than about 3 cm may be suitable for primary excision instead of core biopsy if complete excision with clear margins is achievable and appropriate.
- Discuss anticoagulation management prior to biopsy and weigh bleeding risks against risks of stopping therapy; consider bridging strategies when necessary.
Pathology Role
- Pathologists examine hematoxylin and eosin stained sections and use additional tests to refine or confirm a diagnosis.
- Immunohistochemistry helps determine lineage and narrow differential diagnoses; select panels should be driven by morphology and clinical imaging.
- Molecular tests, including fluorescence in situ hybridization, reverse transcriptase polymerase chain reaction, or next generation sequencing, can confirm characteristic fusion genes or translocations in certain sarcoma subtypes.
- Core biopsy reports may provide subtype and an initial grade, but grading may be revised after resection, when more tumor is available for assessment.
- Report elements for resection specimens should include size, tumor subtype, grade, margin status, and provisional pathological stage.
Multidisciplinary Care Pathway
- Patients with suspected malignant soft tissue tumors should be managed by or discussed in a multidisciplinary team including surgeons, radiologists, pathologists and oncology specialists.
- Local diagnostic multidisciplinary discussion can guide initial imaging, biopsy approach and tissue handling.
- Regional sarcoma multidisciplinary meetings support final treatment planning for confirmed sarcoma, improving diagnostic accuracy and outcomes.
- Avoid unplanned excisions (‘whoops’ procedures) by performing appropriate imaging and biopsy prior to definitive surgery.
Anonymized Case Highlights
- Case A: A superficial foot mass that appeared cystic but proved to be a non-neoplastic infectious process after excision and special staining; illustrates that infections or granulomatous disease can mimic tumors.
- Case B: A rapidly enlarging thigh mass with extensive necrosis; initial core biopsy yielded necrotic material and a diagnostic sample was obtained from an involved lymph node, leading to diagnosis of an aggressive malignancy with characteristic marker loss and prompting timely resection.
- Case C: A mid-leg intramuscular lesion in a young adult; biopsy identified a myxoid liposarcoma subtype that responded to preoperative radiotherapy and required multidisciplinary management including chemotherapy for suspected pulmonary nodules.
Practical Recommendations for Clinicians
- Remember that most soft tissue lumps are benign, but do not assume any lump is benign without appropriate assessment.
- Urgent imaging (for example, ultrasound or magnetic resonance imaging) should be arranged for any unexplained or suspicious lump, following local guidance.
- Use ultrasound as a triage tool for many superficial lumps; proceed to magnetic resonance imaging for deep, large, or indeterminate masses.
- Plan biopsy with the multidisciplinary team so that the pathologist and surgeon are aware of targeting and future resection plans.
- Refer patients with suspected sarcoma to a regional sarcoma center or discuss in a regional multidisciplinary meeting where available.
Key Take-Home Points
- Obtain a careful history and perform a thorough examination for every soft tissue lump.
- Identify red flags early (size > 5 cm, deep location, rapid growth, recurrence, pain) and investigate promptly.
- Employ targeted imaging and image-guided core needle biopsy to maximize diagnostic yield while minimizing harm.
- Multidisciplinary collaboration between clinicians, radiologists, and pathologists is essential for accurate diagnosis and optimal treatment planning.
Leave a Reply