Courtesy: University of Washington Grand Rounds, Harborview, Seattle
Ankle Arthroscopy in Fracture Fixation
Introduction
Ankle arthroscopy is increasingly used as an adjunct to fracture fixation (ORIF).
It plays an important role in:
- Diagnosis
- Treatment
- Prognostication
Historical Background
Early Development
- Kenji Takagi (1918)
- First described arthroscopy (knee, cadaveric)
- Masaki Watanabe
- Introduced fiberoptic arthroscopy
Evolution
Initially, ankle arthroscopy was considered unsuitable due to:
- Narrow joint space
Advances in:
- Small joint instrumentation
- Improved visualization
Led to the widespread adoption of ankle arthroscopy.
Indications of Ankle Arthroscopy
1. Soft Tissue Impingement
Types
- Anterolateral (ATFL / AITFL)
- Anteromedial (deltoid ligament / capsule)
- Posterior (PTFL / posterior capsule)
Treatment
- Debridement or repair
2. Bony Impingement
Causes
- Osteophytes
- Ossicles
Clinical Effect
- Reduced dorsiflexion
Treatment
- Resection
3. Instability
Types
- Lateral ligament injury
- Syndesmotic injury
Role of Arthroscopy
- Detects intra-articular pathology (up to 90%)
- Assists in fixation
4. Osteochondral Lesions
Sites
- Talus
- Distal tibia
Treatment Options
- Debridement
- Microfracture
- Osteochondral grafting
- Chondrocyte implantation
5. Arthritis (Arthrodesis)
Procedure
- Arthroscopic ankle fusion
Advantages
- Less soft tissue damage
Limitations
- Limited deformity correction
6. Other Indications
- Synovitis
- Septic arthritis
- Loose bodies
- Arthrofibrosis
- Diagnostic evaluation (unexplained pain)
- Adjunct in fracture fixation
Contraindications
Absolute
- Local infection
- Severe arthritis with absent joint space
Relative
- Severe edema
- Poor vascular status
- Complex Regional Pain Syndrome
Technique Essentials
Equipment
- Arthroscope: 1.9–2.7 mm
- Optics: 30° or 70°
- Small shavers and probes
Distraction
Purpose
- Improves visualization
Types
- Non-invasive (preferred)
- Invasive (less commonly used)
Limits
- Less than 30 lbs force
- Less than 1 hour duration
Portal Placement
Anteromedial Portal
- Medial to tibialis anterior tendon
Anterolateral Portal
- Lateral to peroneus tertius tendon
Key Risk
- Injury to superficial peroneal nerve
Complications
Incidence
- Approximately 3.4–17%
Common Complications
- Neurovascular injury (most common)
- Infection
- Arthrofibrosis
- Instrument breakage
- Pulmonary embolism
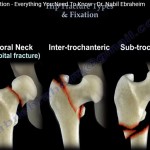
Ankle Fractures Overview
Common Patterns
- Unimalleolar
- Bimalleolar
- Trimalleolar
Classification Systems
- Lauge–Hansen (mechanism-based)
- Danis–Weber (fibular level-based)
Outcomes in Ankle Fractures
Key Determinant
- Quality of reduction
Good Reduction
- Approximately 80% good outcomes
Poor Reduction
- Approximately 25% good outcomes
Important Factor
- Associated cartilage injury worsens prognosis
Role of Arthroscopy in Fractures
Primary Goals
- Identify chondral injuries
- Remove loose bodies
- Assess syndesmotic reduction
- Aid prognostication
Evidence from Literature
Cartilage Injury
- Present in approximately 60–80% of ankle fractures
Higher Risk Patterns
- Weber C fractures
- Syndesmotic injuries
- Fracture dislocations
RCT Findings
- Mixed results
- Some studies show slight functional improvement
- Overall evidence remains inconclusive
Key Practical Indications
1. Loose Bodies
Incidence
- Present in approximately 55% of fractures
Clinical Impact
- Joint locking
- Early arthritis
Role of Arthroscopy
- Effective removal
2. Fracture Dislocations
Clinical Significance
- Very high risk of cartilage injury
Indication
- Strong indication for arthroscopy
- Especially in young, active patients
3. Syndesmotic Injuries
Problem
- Malreduction rates up to 40%
Role of Arthroscopy
- Direct visualization
- Detection of diastasis
- Dynamic assessment of reduction
Assessment of Syndesmosis
Available Methods
- Contralateral X-rays
- Intraoperative open assessment
- 3D imaging (most accurate)
- Arthroscopy (adjunct tool)
Limitations of Arthroscopy
- Increased operative time
- Higher cost
- Risk of complications
- Not required in all cases
Clinical Decision-Making
Indications for Arthroscopy
- Young, active patients
- Fracture dislocations
- Suspected cartilage injury
- Syndesmotic injury
- Presence of loose bodies
When to Avoid
- Open fractures
- Poor soft tissue condition
- Elderly or low-demand patients
- Severe swelling
Real-World Practice
- Approximately 20% of ankle fractures undergo arthroscopy
- Used selectively rather than routinely
Key Exam Pearls
- Cartilage injury occurs in 60–80% of ankle fractures
- Fracture dislocations have the highest risk
- Arthroscopy is both diagnostic and therapeutic
- Syndesmotic reduction is frequently inaccurate
- Arthroscopy improves assessment but is not the gold standard
- Use is selective, not routine
Take-Home Message
- Arthroscopy is a valuable adjunct, not mandatory
- Best used in:
- High-risk fracture patterns
- Situations with diagnostic uncertainty
Benefits
- Improves diagnostic accuracy
- Guides surgical treatment
- Assists in patient counselling

i am a master student in traumatic surgery and I am interest in orthopedics