Courtesy: Prof Nabil Ebraheim, University of Toledo, Ohio, USA
Overview
Pediatric elbow fractures broadly include:
- Supracondylar fractures of the humerus
- Fractures involving ossification centres
This section focuses on fractures involving ossification centres.
Ossification Centres of the Elbow
Understanding timing is critical for diagnosis.
Elbow ossification centers CRITOE
| Structure | Age (years) |
|---|---|
| Capitellum | 1 |
| Radial head | 3 |
| Medial epicondyle | 5 |
| Trochlea | 7 |
| Olecranon | 9 |
| Lateral epicondyle | 11 |
1. Transepiphyseal Separation of Distal Humerus
Key Clinical Points
- Seen in very young children, often below 1 year
- Strongly consider non-accidental injury
Differentiation from Elbow Dislocation
| Feature | Elbow Dislocation | Transepiphyseal Separation |
|---|---|---|
| Age | Older children | Infants |
| Displacement | Posterolateral | Posteromedial |
| Radiocapitellar line | Disrupted | Maintained |
Key Diagnostic Point
- If the radiocapitellar line is intact and radial head aligns with capitellum, diagnosis favors transepiphyseal separation
Clinical Importance
- Often missed
- High suspicion required in infants with elbow injury
2. Lateral Condylar Fracture of Humerus
Classification
- Typically Salter-Harris classification Type IV
Key Points
- Appears nondisplaced on standard views
- Internal rotation view may reveal displacement
Management
- Requires close follow-up if treated conservatively
- Most cases are displaced and require surgery
Surgical Principle
- Use lateral approach
- Avoid posterior approach
- Risk of avascular necrosis of capitellum
Complications
1. Non-union
- Leads to cubitus valgus deformity
2. Ulnar Nerve Symptoms
- Develop over time due to stretch from valgus deformity
Treatment of Complications
- Non-union with pain: bone grafting and fixation
- Ulnar nerve symptoms: decompression or transposition
Key Exam Point
- Lateral condylar fracture is considered a surgical fracture
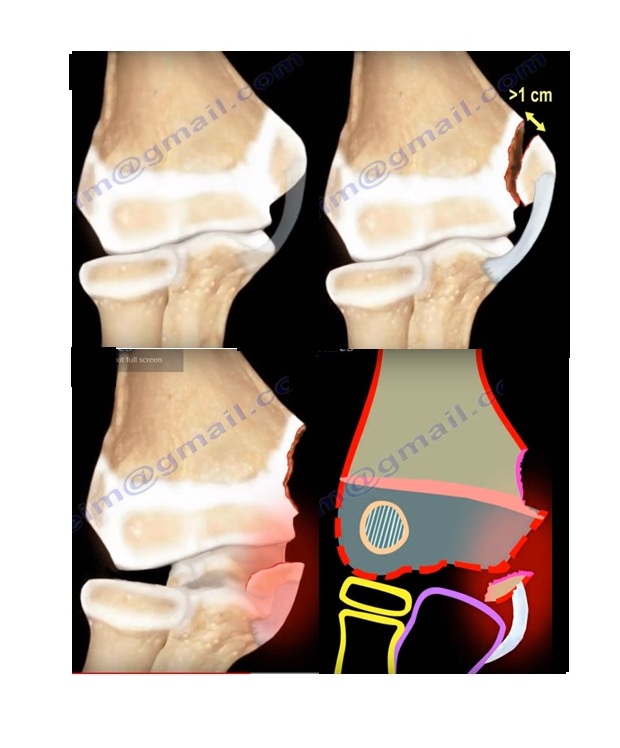
3. Medial Epicondyle Fracture
Key Points
- Last ossification centre to fuse
- Commonly associated with elbow dislocation
Management
- Usually treated conservatively
Indications for Surgery
- Displacement greater than 1 cm (controversial)
- Fragment trapped within the joint
Important Step
- Always check for medial epicondyle on post-reduction X-ray
4. Radial Head and Neck Fractures
Management Criteria
- Less than 30 degrees angulation: conservative treatment
If Displacement is Greater Than 30 Degrees
- Closed reduction
If Reduction is Difficult
- Percutaneous pin used as joystick
Indication for Open Reduction
- Residual angulation greater than 45 degrees
Complications
1. Synostosis
- Fusion between radius and ulna
- May be due to periosteal interposition
2. Osteonecrosis
- Due to disruption of blood supply
3. Loss of Motion
- Common complication
4. Non-union (Rare)
- May be due to periosteal interposition
5. Compartment Syndrome
- Must be actively monitored
Key Radiological Rule
- Radiocapitellar line must pass through the capitellum in all views
High-Yield Exam Pearls
- Elbow dislocation is rare in infants, suspect transepiphyseal separation
- Lateral condylar fracture has high risk of non-union and deformity
- Medial epicondyle fragment may be trapped inside the joint
- Radial head fractures should avoid open reduction when possible
- Always correlate age with ossification centres
- Always assess radiocapitellar alignment
Final Takeaway
- Pediatric elbow injuries require:
- Knowledge of ossification sequence
- Careful radiographic interpretation
- High suspicion for subtle injuries
- Missing these injuries can lead to:
- Deformity
- Nerve complications
- Long-term functional impairment


Leave a Reply