Courtesy: Prof Shital Parikh MD, Cincinnati Childeren’s Hospital, Philadelphia, PN
Part 1: Fracture Mimickers in Children
1. Irregular Ossification – A Common Trap
-
Pediatric ossification centers are irregular and may mimic fractures.
-
The elbow is particularly challenging due to multiple ossification centers.
-
Familiarity with:
-
Order of appearance
-
Timing of fusion
-
Normal variants
is essential to avoid misdiagnosis.
-
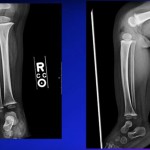
Key Strategy:
-
When in doubt, obtain a contralateral X-ray for comparison.
2. Multi-Partite Apophysis
-
Olecranon may ossify from multiple centers.
-
Can resemble fracture in acute trauma.
-
Bilateral comparison helps differentiate normal from fracture.
3. Lateral Epicondyle Ossification
-
Appears transiently.
-
May mimic fracture on lateral view.
-
Short window of visibility ? easily mistaken.
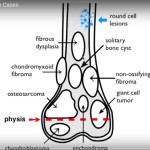
4. Irregular Ossification vs Osteochondritis Dissecans (OCD)
Seen commonly in the distal femur.
Differentiation Based on Age:
-
< 8 years ? usually irregular ossification
-
12 years ? usually OCD
-
8–12 years ? grey zone (clinical judgment + MRI)
MRI Clues for Irregular Ossification:
-
No cartilage breach
-
No fluid beneath lesion
-
Tends to resolve with observation
5. Patella Variants
-
Normal irregular patellar ossification
-
Bipartite patella (often superolateral and bilateral)
-
Dorsal defect of patella (benign)
May mimic:
-
Osteomyelitis
-
Osteochondral fracture
6. Epiphyseal Variants
Possible normal findings:
-
Cleft epiphysis
-
Double epiphysis
-
Pseudo-epiphysis
-
Notched epiphysis
-
Wedge-shaped epiphysis
-
Undulating physis
Rotation of limb can create illusion of fracture lines.
7. Fifth Metatarsal Apophysis
-
Apophysis runs longitudinally.
-
Fracture line runs transversely.
-
Orientation helps distinguish fracture from normal apophysis.
8. Accessory Ossicles
Common around:
-
Ankle
-
Foot
-
Wrist
Examples:
-
Os peroneum
-
Medial malleolar ossicle
-
Bipartite navicular
These may be:
-
Normal variants
-
Or fractures through accessory ossicle
Clinical correlation is essential.
9. Growth Variants
-
Supracondylar spur (points toward elbow; unlike osteochondroma)
-
Postero-medial distal femoral irregularity
-
Deltoid insertion irregularity
-
Dorsal patellar defect
Often mistaken for tumors.
10. Nutrient Channels
-
Can resemble hairline or greenstick fractures.
-
Must differentiate carefully.
11. Infection or Tumor Mimicking Fracture
Red Flags:
-
Fever
-
Increasing swelling
-
Systemic illness
-
Disproportionate symptoms
Cases discussed:
-
Osteomyelitis following trivial trauma
-
Osteosarcoma initially diagnosed as fracture
Clinical suspicion is critical.
12. Non-Accidental Trauma (Child Abuse)
Must consider in:
-
Infants
-
Multiple fractures
-
Fractures at different stages of healing
-
Rib, scapular, distal clavicle fractures
-
Corner or bucket-handle metaphyseal fractures
Important:
-
Avoid both under-diagnosis and over-diagnosis
-
Consider metabolic or collagen disorders
Part 2: Missed Fractures in Children
Prospective data showed:
-
~10% error rate in pediatric fracture interpretation.
-
High discordance between ED physician and radiologist readings.
Commonly Missed Areas:
-
Ankle
-
Foot
-
Wrist
-
Hand
-
Elbow
Distal Tibia & Ankle Injuries
-
Intra-articular fractures often underestimated on X-ray.
-
CT scan changes:
-
Fracture pattern (46%)
-
Measured displacement (39%)
-
Treatment plan (25%)
-
Low Threshold for CT:
-
Transitional fractures
-
Salter-Harris III & IV
-
Intra-articular injuries
Complex Tibial Shaft + Intra-Articular Fracture
-
Focus on obvious shaft fracture may lead to missed ankle fracture.
-
CT scan essential in suspicious cases.
Deep MCL Avulsion
-
May appear as small fragment.
-
Persistent pain despite conservative treatment.
-
Surgical fixation may be required.
Missed Osteochondral Fractures
-
Particularly after patellar dislocation.
-
Cartilage fragments may be hidden in posterior gutter.
-
MRI essential for diagnosis.
Tibial Spine (ACL Avulsion) – Cartilaginous Injuries
-
May not be visible on X-ray.
-
MRI shows displaced cartilaginous avulsion.
-
Late diagnosis complicates management.
Bipartite Patella vs Osteochondral Fracture
-
Bipartite usually superolateral and bilateral.
-
True fracture correlates with mechanism and symptoms.
Proximal Tibial Posterior Fractures
-
Subtle on X-ray.
-
Risk of:
-
Vascular injury
-
Compartment syndrome
-
MRI helpful.
Seymour Fracture (Distal Phalanx)
-
Open physeal fracture.
-
Nail plate lies over nail fold (not under).
-
Requires:
-
Nail removal
-
Debridement
-
Reduction
-
Nail bed repair
-
Antibiotics
-
Complications if missed:
-
Osteomyelitis
-
Nail deformity
-
Growth arrest
Phalangeal Neck & Condylar Fractures
-
May remodel, but improper treatment causes:
-
Deformity
-
Contracture
-
Motion restriction
-
Clinical examination (finger cascade) is essential.
Elbow “TRASH” Lesions
(Trauma Radiographic Appearance Seems Harmless)
Commonly Missed:
-
Monteggia fractures
-
Radial head fractures
-
Medial epicondyle incarceration
-
Coronoid fractures
-
Lateral condyle fractures
Posterior Fat Pad Sign
-
Always abnormal.
-
Suggests intra-articular injury.
Monteggia Injury
-
Look for radial head alignment.
-
Draw line along radial shaft ? must intersect capitellum.
-
Always evaluate radio-capitellar relationship.
Missed Monteggia ? complex reconstructive surgery.
Radial Head Fractures
-
Can progress to:
-
Posterior subluxation
-
Rapid arthritis
-
Late cases may require radial head excision.
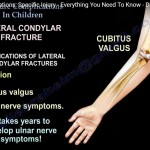
Medial Condyle Fracture
-
May rotate 180° if missed.
-
Requires surgical fixation.
Coronoid Fracture
-
Provides elbow stability.
-
Often cartilaginous in younger children.
-
Requires fixation if unstable.
Arthrogram for Lateral Condyle Fractures
-
Helps assess articular hinge.
-
Determines need for open reduction.
Transphyseal Fracture vs Elbow Dislocation
-
Radio-capitellar alignment intact ? transphyseal fracture.
-
Both relationships disrupted ? dislocation.
Imaging Strategy Summary
CT Scan
Indicated for:
-
Intra-articular fractures
-
Transitional fractures
-
Surgical planning
MRI
Indicated for:
-
Cartilaginous injuries
-
Osteochondral lesions
-
Ligament avulsions
-
Pre-ossified epiphysis injuries
Role of Artificial Intelligence
Study showed:
-
AI improved detection sensitivity from 77% to 98%.
-
May reduce ED diagnostic errors.
Future role likely significant in pediatric trauma imaging.
Final Key Messages
-
Pediatric bones have many normal variants.
-
Always correlate clinically.
-
Compare with contralateral side when unsure.
-
Maintain high suspicion for:
-
Infection
-
Tumor
-
Non-accidental trauma
-
-
Use CT for intra-articular fractures.
-
Use MRI for cartilaginous injuries.
-
Always check radio-capitellar alignment.
-
Do not ignore subtle findings.
Most Important Principle:
The child should not suffer due to missed or misdiagnosed injuries.
Leave a Reply