Courtesy: Prof Nabil Ebraheim, University of Toledo, Ohio, USA
ANATOMY OF THE ULNAR ARTERY
- The brachial artery divides at the neck of the radius into two branches: the radial artery and the ulnar artery.
- The ulnar artery is the largest of the two branches. Initially, it descends obliquely crossing part of the brachialis and the flexor digitorum profundus.
- Four muscles that arise from the medial epicondyle will cross the oblique part over the artery and these are the following muscles:
The Pronator Teres
The Flexor Carpi Radialis The palmaris longus
The Flexor Digitorum superficialis - The obliquepart of the ulnar artery then turns vertically on the ulnar aspect of the forearm (the medial aspect).
- The vertical part of the artery is partially covered by the flexor carpi ulnaris.
- In the distal part of the forearm, the artery becomes superficial, and the ulnar nerve is ulnar to the artery.
- The flexor carpi ulnaris is medial to the artery and laterally you find the flexor digitorum superficialis.
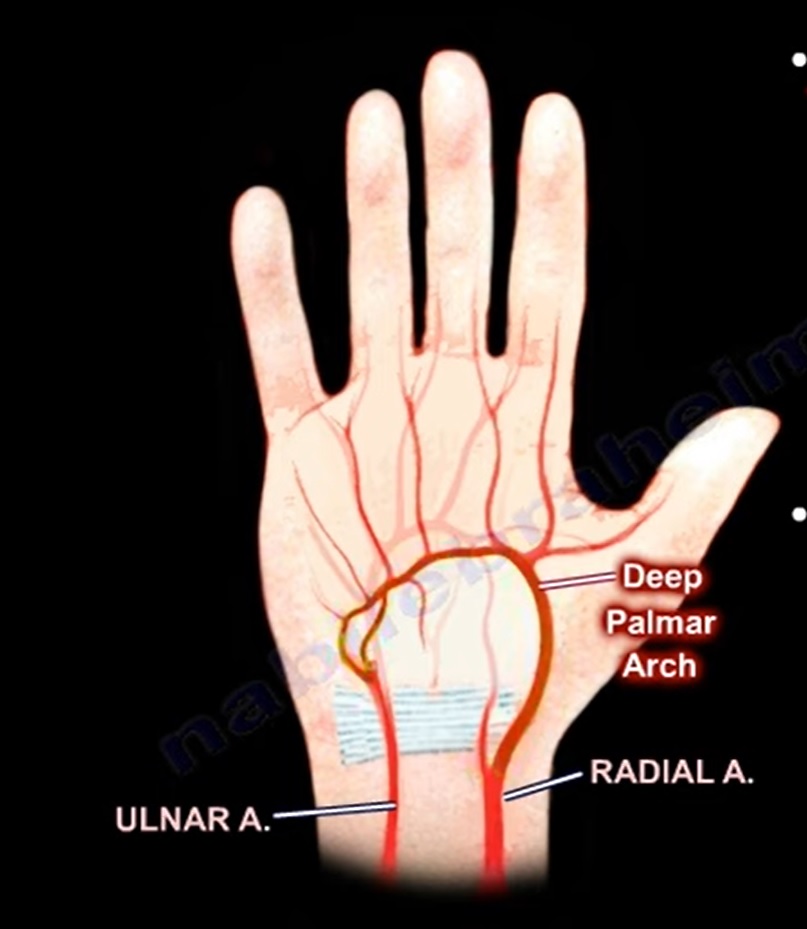
- At the wrist, the ulnar artery goes superficial to the flexor retinaculum, and it makes the superficial palmar arch after it enters the hand.
So what are the branches of the ulnar artery?
- The ulnar artery gives muscular branches and it gives the ulnar recurrent artery, anterior and posterior.
- The anterior ulnar recurrent artery passes in front of the medial epicondyle of the humerus.
- The posterior ulnar recurrent artery passes posterior to the medial epicondyle of the humerus.
- The anterior and posterior ulnar recurrent arteries arise near the elbow and ascend to anastomose with branches of the brachial artery in front of and behind the medial epicondyle.
- The anterior ulnar recurrent artery will have anastomosis with the inferior ulnar collateral artery.
- The posterior ulnar recurrent artery will make an anastomosis with the superior collateral artery.
- After the ulnar recurrent arteries, the common interosseous artery appears, which is one inch below its beginning and divides into anterior and posterior branches.
- The branches of the common interosseous artery are named as they relate to the interosseous membrane anteriorly and posteriorly.
- The anterior interosseous artery is the largest range and it runs downwards over the anterior surface of the interosseous membrane between the flexor pollicis longus and the flexor digitorum profundus.
- The anterior interosseous artery also supplies the deep muscle of the anterior compartment of the forearm including the flexor digitorum profundus, the flexor pollicis longus and the pronator quadratus.
- The anterior interosseous artery ends by joining the posterior carpal arch.
- The anterior interosseous artery gives a branch called the median artery, which accompanies the median nerve and nutrient branches to the radius and ulna.
- The posterior interosseous artery is the smallest branch. It passes backwards above the interosseous membrane to reach the back of the forearm where it runs downwards between the superficial and deep muscles of the back of the forearm.
- The posterior interosseus artery will supply the extensor compartment of the forearm and will give a branch called the interosseous recurrent branch which enters into the anastomosis at the posterior aspect of the lateral epicondyle.
- After the common interosseous artery, the ulnar artery will give anterior and posterior carpal branches.
- The ulnar artery will anastomose with the carpal branches of the radial artery to form the anterior and posterior carpal arches.
- The ulnar artery will give a deep branch which will anastomose with the radial artery to make the deep palmar arch.
- The deep palmar arch is formed predominantly by the radial artery.
- The radial artery ends by being a continuation of the radial artery, and will give the deep palmar arch.
The Superficial Branch: The ulnar artery ends by being the superficial palmar arch, which gets contribution from the radial artery through the superficial palmar branch of the radial artery.
The deep and superficial palmar arch names come from their relationship to the long flexor tendons in the hand.
The Deep Palmar Arch lies deep to the long flexor tendons.
The Superficial Palmar Arch lies superficial to the long flexor tendons.
- The Deep palmar arch lies one finger breadth distal to the distal crease of the forearm.
- The Superficial Palmar Arch lies two-finger breadths distal to the distal crease of the forearm.
- The most distal point is at the level of the distal border of the fully abducted thumb.
What are the branches of the ulnar artery?
• Anterior ulnar recurrent artery
• Posterior ulnar recurrent artery
• Common interosseous artery
• Carpal branches
• Deep Palmar branch
The profunda brachii with the ulnar artery
The post-terminal branch of the profunda brachii anastomose with the posterior interosseous recurrent artery. The posterior interosseous recurrent artery runs behind the lateral epicondyle and it is a branch of the posterior interosseous artery.


Leave a Reply