Courtesy: Prof Nabil Ebraheim, University of Toledo, Ohio, USA
Superior Gluteal Artery
Overview
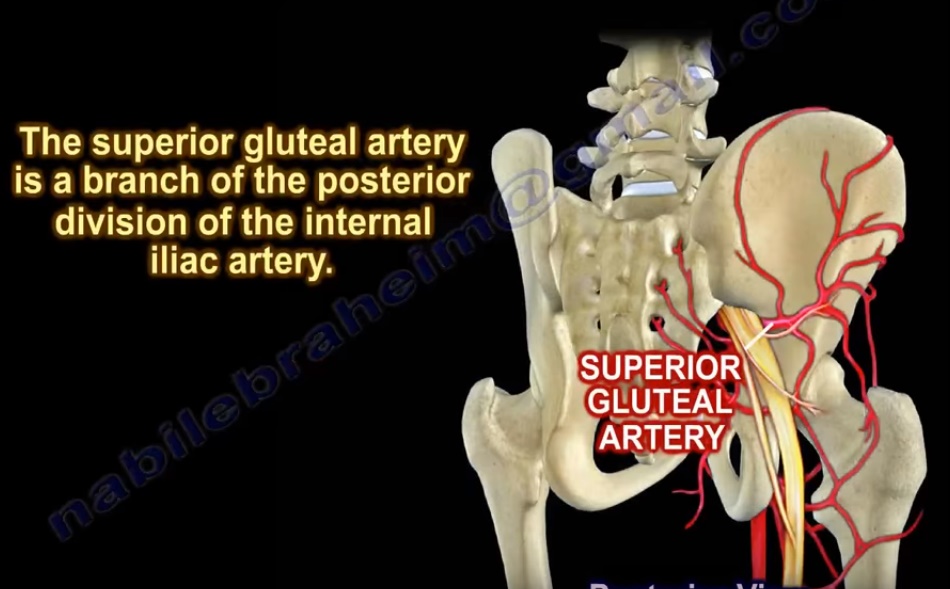
The superior gluteal artery is the largest branch of the internal iliac artery.
Clinical Importance
- Injury can cause massive hemorrhage
- At risk in:
- Pelvic fractures
- Acetabular surgery
- Damage may lead to:
- Gluteal muscle ischemia
Origin
Arterial Pathway
- Abdominal aorta divides at L4 into:
- Right common iliac artery
- Left common iliac artery
- Each common iliac artery divides into:
- External iliac artery
- Internal iliac artery
Source of Superior Gluteal Artery
- Arises from:
- Posterior division of internal iliac artery
Course
The artery follows this pathway:
- Exits pelvis through greater sciatic foramen
- Passes above the piriformis muscle
- Enters the gluteal region
Branches
1. Superficial Branch
Course
- Between:
- Gluteus maximus
- Gluteus medius
Supply
- Gluteus maximus
- Overlying skin
2. Deep Branch
Course
- Between:
- Gluteus medius
- Gluteus minimus
- Lies on deep surface of gluteus medius
Supply
- Gluteus medius
- Gluteus minimus
- Tensor fascia lata
Comparison: Inferior Gluteal Artery
Origin
- Anterior division of internal iliac artery
Course
- Exits pelvis:
- Below piriformis
Supply
- Gluteus maximus
- Posterior thigh
Key Difference
| Artery | Relation to Piriformis |
|---|---|
| Superior gluteal artery | Above |
| Inferior gluteal artery | Below |
Additional Branches
- Sciatic artery (vasa nervorum) — supplies sciatic nerve
- Anastomotic branches — contribute to cruciate anastomosis
Clinical Importance
1. Posterior Iliac Crest Bone Graft
Risk
- Extension into greater sciatic notch may injure artery
Consequence
- Severe hemorrhage
2. Extended Iliofemoral (Letournel) Approach
Used For
- Complex acetabular fractures
Key Point
- Gluteal muscles remain attached mainly via:
- Superior gluteal artery
Risk of Injury
- Devitalization of gluteal muscles
- Muscle necrosis
3. Pelvic Fractures
Sources of Bleeding
- Venous (most common)
- Bone
- Arterial (~10%)
Injuries Associated With
- Sacroiliac joint disruption
- Anteroposterior compression injuries
- Shear injuries
Complications
- Massive hemorrhage
- Hypovolemic shock
Massive Transfusion Protocol
Ratio
- 1 : 1 : 1
Components
- Packed RBC
- Fresh frozen plasma
- Platelets
Diagnosis of Arterial Injury
Investigations
- CT angiography
- Pelvic angiography
Indication for Angiography
- Persistent hemodynamic instability
- Despite >/= 4 units blood transfusion in first hour
Treatment
Angiographic Embolization
- Effective method to control bleeding
- Superior gluteal artery can be embolized
Surgical Risk
At Risk During
- Screw placement near sciatic notch
- Acetabular fracture fixation
Precaution
- Palpate sciatic notch
- Avoid screw penetration
Management of Intraoperative Injury
Steps
- Attempt arterial clipping
- Avoid injury to superior gluteal nerve
- Perform packing
- Call:
- Vascular surgeon
- Interventional radiologist
- Ensure adequate blood transfusion
Key Exam Points
Origin
- Posterior division of internal iliac artery
Exit
- Greater sciatic foramen (above piriformis)
Supply
- Gluteus maximus
- Gluteus medius
- Gluteus minimus
- Tensor fascia lata
Clinical Relevance
- Pelvic fracture hemorrhage
- Iliac crest graft complications
- Acetabular surgery risk
- Sciatic notch screw placement

Leave a Reply