Courtesy: Michael Bullen and the OrthoFRACS
Rickets: Causes, Pathophysiology, and Management
Overview
Rickets is a pediatric metabolic bone disorder characterized by:
- Defective mineralization of:
- Growth plate cartilage
- Bone
- Skeletal deformities
- Growth retardation
Most Common Cause
- Vitamin D deficiency
Historical Notes
- Term derived from German word “Ricken” (meaning twisted)
- Known as the “English disease”
- Early description by Francis Glisson
Epidemiology
- Previously common during industrial revolution (low sunlight exposure)
- Now:
- Decreasing in developed countries
- Re-emerging globally
High-Risk Groups
- Limited sunlight exposure
- Dark-skinned individuals in low sunlight regions
Global Burden
- Remains common in developing countries
Vitamin D Metabolism
Step 1: Skin
- UVB converts:
- 7-dehydrocholesterol — Cholecalciferol (Vitamin D3)
Step 2: Liver
- Cholecalciferol —} 25-hydroxyvitamin D (Calcidiol)
Step 3: Kidney
- Calcidiol —} Calcitriol (active form)
Key Point
- Defect at any step —} Rickets
Functions of Vitamin D
Intestine
- Increases calcium and phosphate absorption
Bone
- Promotes mineralization
Kidney
- Reduces calcium and phosphate excretion
In Deficiency
- Decrease in Calcium absorption
- Increased parathyroid Parathyroid hormone
- Increased Bone resorption
Definition of Vitamin D Deficiency
Best Marker
- Serum 25-hydroxyvitamin D
Levels
| Level | Interpretation |
|---|---|
| <25 nmol/L | High risk for rickets |
| <50 nmol/L | Vitamin D insufficiency |
Causes of Rickets
1. Maternal / Perinatal
- Maternal deficiency
- Prematurity
2. Nutritional
- Exclusive breastfeeding without supplementation
- Poor dietary intake
- Restricted diets
3. Environmental
- Limited sunlight exposure
- Dark skin in low sunlight regions
- Cultural clothing limiting sun exposure
Pathophysiology
Sequence
- Decreased Calcium absorption
- Increased Parathyroid hormone
- Increased Phosphate loss (kidney)
- Impaired mineralization
Outcome
- Accumulation of osteoid
- Weak, deformable bones
- Growth plate abnormalities
Types of Rickets
1. Nutritional Rickets
- Deficiency of:
- Vitamin D
- Calcium
- Phosphate
2. Vitamin D–Dependent Rickets
- Type I:
- 1-alpha hydroxylase deficiency
- Type II:
- Vitamin D receptor resistance
3. Vitamin D–Resistant Rickets
Most Common
- X-linked hypophosphatemic rickets
Features
- Renal phosphate wasting
- X-linked dominant inheritance
Clinical Evaluation
History
- Sunlight exposure
- Diet
- Growth and development
- Family history
- Consanguinity
- Dental issues
Symptoms of Hypocalcemia
- Muscle cramps
- Paresthesia
- Seizures
Clinical Features
Age Group
- Infancy
- Early childhood
- Adolescence
Skeletal Features
- Bowing of long bones
- Growth delay
- Kyphosis
- Gait abnormalities
Characteristic Signs
Rachitic Rosary
- Enlargement of costochondral junctions
Other Signs
- Frontal bossing
- Delayed fontanelle closure
Spine
- Codfish vertebrae
Other Features
- Dental abnormalities
- Pathological fractures
Looser Zones (Pseudofractures)
- Incomplete stress fractures
- Occur on compression side of bone
Investigations
Blood Tests
- Calcium
- Phosphate
- Alkaline phosphatase
- Parathyroid hormone
- 25-hydroxyvitamin D
- Renal function
Urine Tests
- Urinary calcium
- Urinary phosphate
Typical Lab Findings (Nutritional Rickets)
| Test | Finding |
|---|---|
| Calcium | Low / normal |
| Phosphate | Low |
| Vitamin D | Low |
| ALP | High |
| PTH | High |
| Urinary phosphate | High |
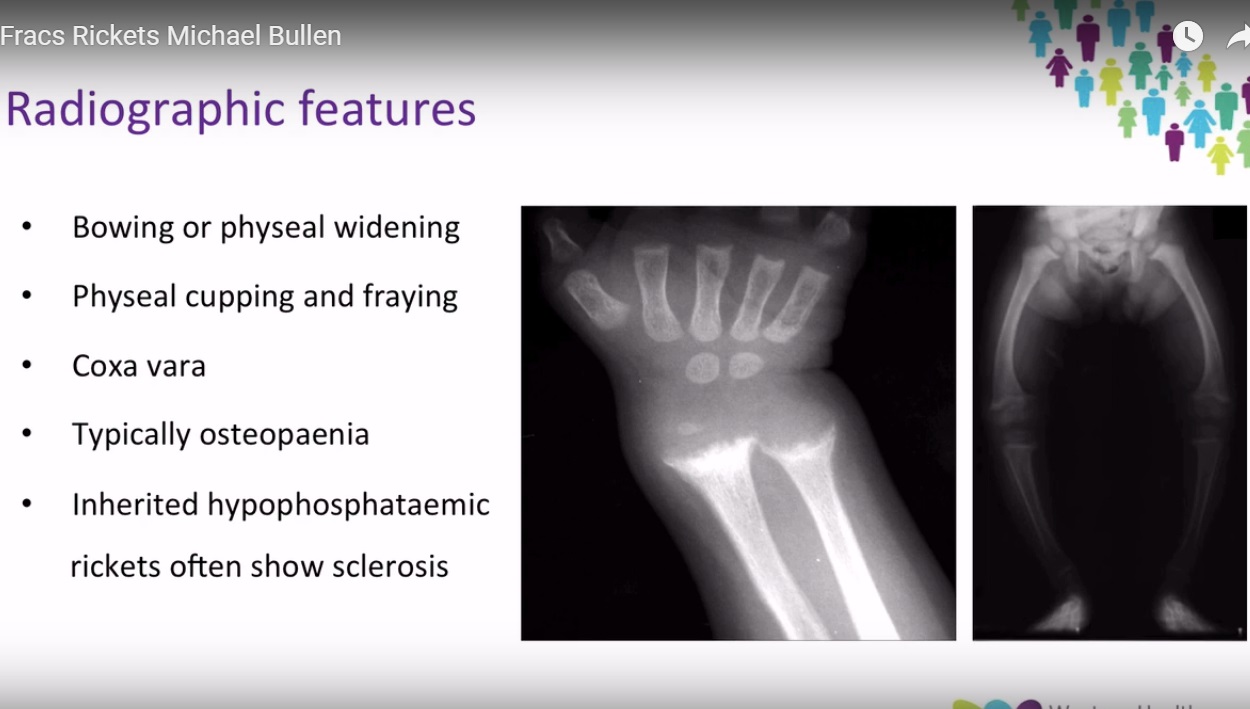
Radiographic Features
Classic Findings
- Metaphyseal widening
- Cupping
- Fraying
- Bowing deformities
- Osteopenia
Common Sites
- Wrist (distal radius)
- Distal femur
- Proximal tibia
Additional
- Rachitic rosary
- Delayed bone age
Fracture Risk
- Vitamin D correlates with bone density
- Bone may be:
- Dense beneath osteoid
- But structurally weak
Treatment
Primary Treatment
- Vitamin D supplementation
Options
- Cholecalciferol
- Ergocalciferol
- Calcitriol
Routes
- Oral
- Intramuscular
Example
- Single high dose (e.g., 150,000 IU)
Response to Treatment
- Radiographic improvement:
- Within 1 week
- Healing:
- ~6 weeks
- Deformity correction:
- Months
Surgical Management
Rarely Required
Indications
- Severe deformity
- Failure of medical treatment
Important Rule
- Correct metabolic abnormality before surgery
Key Exam Points
- Rickets = defective mineralization at growth plate
- Best marker = 25-hydroxyvitamin D
- Classic X-ray:
- Cupping
- Fraying
- Widening
- Classic sign:
- Rachitic rosary
- Treatment:
- Vitamin D supplementation

Leave a Reply