Courtesy: Prof Nabil Ebraheim, University of Toledo, Ohio, USA
Osteoporosis: Causes, Pathophysiology, and Clinical Impact
Overview
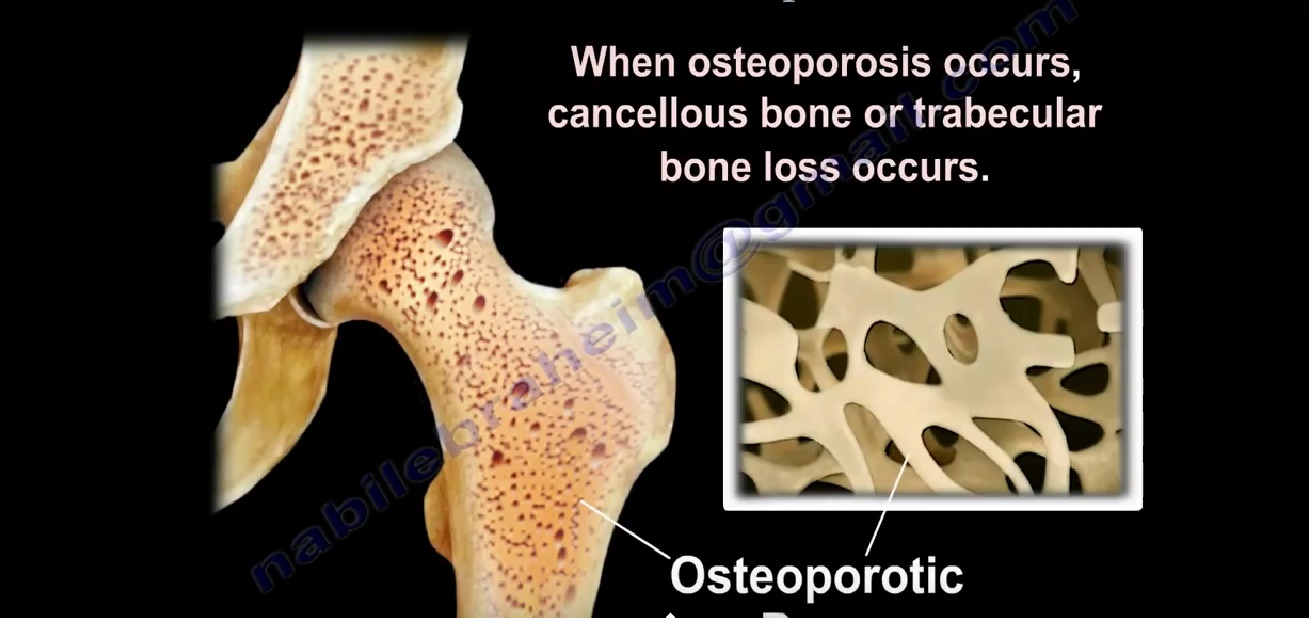
Osteoporosis is a common skeletal disorder characterized by:
- Decreased bone mass
- Deterioration of bone microarchitecture
- Reduced bone strength
Leads to an increased risk of fractures
Bone Strength Depends On
- Bone mineral density (BMD)
- Bone quality:
- Microarchitecture
- Bone turnover
- Mineralization
Common Osteoporotic Fractures
Typical Sites
- Distal radius (wrist)
- Vertebral spine
- Hip
Age-Related Pattern
- Younger postmenopausal women:
- Wrist fractures first
- Elderly:
- Hip fractures more common
Risk of Subsequent Fractures
After Vertebral Fracture
- -5× increased risk of:
- Another vertebral fracture
- Increased risk of:
- Hip fracture
After Hip Fracture
- 8–10× increased risk of:
- Second hip fracture
Important Clinical Insight
- Higher mortality in men after hip fracture compared to women
Mortality Associated with Osteoporosis
- 20–25% of elderly patients die within 1 year after hip fracture
Common Causes
- Immobility
- Infection
- Thromboembolism
Lifetime Risk of Fracture
- Women: -40–50%
- Men: -13–22%
Bone Physiology
Bone Remodeling Cells
Osteoclasts
- Function:
- Bone resorption
- Remove old bone
Osteoblasts
- Function:
- Bone formation
- Produce new bone matrix
Normal Bone Balance
- Bone health depends on balance between:
- Resorption (osteoclasts)
- Formation (osteoblasts)
Pathophysiology of Osteoporosis
Key Mechanism
- Bone mineralization: Normal
- Problem:
- Reduced bone mass (quantity)
Result
- Increased osteoclastic activity
OR - Decreased osteoblastic activity
Outcome
- Progressive bone loss
- Structural weakening
Important Concept
- Osteoporosis is a quantitative bone disorder
- Not a defect in mineralization
Osteoporosis vs Osteomalacia
| Feature | Osteoporosis | Osteomalacia |
|---|---|---|
| Primary problem | Decreased bone mass | Defective mineralization |
| Mineralization | Normal | Reduced |
| Bone structure | Thin trabeculae | Soft bone |
| Common cause | Aging, menopause | Vitamin D deficiency |
Peak Bone Mass
- Achieved between:
- 16–25 years
Clinical Importance
- Higher peak bone mass — lower fracture risk later
Age-Related Bone Loss
In Men
- Begins after -25 years
- Rate: -0.3% per year
In Women
- Rate: -0.5% per year
Postmenopausal Bone Loss
Cause
- Estrogen deficiency
Rate
- 2–3% per year
Duration
- Rapid phase lasts:
- 5–10 years
Types of Osteoporosis
Type I – Postmenopausal Osteoporosis
Features
- Occurs 15–20 years after menopause
- Caused by estrogen deficiency
- Affects:
- Trabecular bone
Common Fractures
- Vertebral fractures
- Wrist fractures
Type II – Senile Osteoporosis
Features
- Occurs after age 70
- Affects both sexes
- Causes:
- Aging
- Calcium & vitamin D deficiency
Bone Involvement
- Cortical + trabecular bone
Common Fractures
- Hip fractures
- Vertebral fractures
Structural Changes in Aging Bone
- Increased medullary cavity
- Reduced cortical thickness
Leads to reduced mechanical strength
Epidemiology
- Affects:
- 45–50% of women >50 years
- Lower but significant in men
Gender Ratio
- Female : Male –2 : 1
Risk Factors for Osteoporosis
Non-Modifiable Factors
- Female sex
- Increasing age
- Family history
- Caucasian / Northern European ancestry
- Low body weight
Lifestyle Factors
- Sedentary lifestyle
- Smoking
- Excess alcohol
- Poor calcium / vitamin D intake
Medication-Related Factors
- Long-term use of:
- Glucocorticoids
- Anticonvulsants (e.g., phenobarbital)
- Other drugs affecting bone metabolism
Key Takeaways
- Osteoporosis is a silent disease until fracture occurs
- Bone mineralization is normal — problem is loss of bone mass
- Hip fractures carry high mortality
- Peak bone mass in youth is critical for prevention
- Early identification of risk factors is essential

Leave a Reply