Courtesy: Koswhik Jain, FRCS Orth, Dudley Group, NHS Trust, UK
Total Ankle Replacement (TAR): Overview, Principles, and Clinical Practice
Overview
Total Ankle Replacement (TAR) is an evolving surgical procedure for end-stage ankle arthritis, aimed at:
- Pain relief
- Preservation of ankle motion
- Improved gait mechanics
Despite increasing adoption, TAR remains a relatively less common and technically demanding procedure, with ongoing debate regarding indications and outcomes
Epidemiology and Current Trends
Global Perspective
- TAR is far less common than hip or knee replacement
- Example (UK data):
- ~100,000 hip/knee replacements annually
- ~800–900 ankle replacements per year
Trend
- Gradual increase in TAR procedures
- Still considered a specialized (niche) surgery
Historical Background
- Successful hip replacement pioneered by Sir John Charnley (1940s)
- First ankle replacements attempted in the 1970s
- Early designs used hip prostheses
- High failure rates
Evolution
- Multiple implant generations developed
- TAR remains less standardized compared to hip and knee arthroplasty
Principles of Total Ankle Replacement
Successful TAR depends on:
Alignment
- Components aligned perpendicular to the mechanical axis
Stability
- Balanced ankle (medial and posterior stability)
Congruity
- Proper joint surface matching
Motion
- Adequate range of motion
- Avoid overly tight or loose constructs
Implant Design Considerations
Cemented vs Uncemented
- UK: predominantly uncemented implants
- USA: mostly cemented implants (regulatory differences)
Fixed-Bearing vs Mobile-Bearing
Fixed-Bearing
- Example: Infinity TAR
- Advantages:
- Lower risk of dislocation
- Disadvantage:
- Increased stress on tibial component
Mobile-Bearing
- Examples: Zenith, Mobility
- Advantages:
- Mimics natural ankle motion
- Disadvantages:
- Risk of bearing dislocation
Key Point
- No definitive evidence proving superiority of one design
Outcomes (Registry Data)
- TAR volume increased significantly over the last decade
- Temporary drop during COVID-19
Revision Risk
- ~8.5% at 10 years (UK registry)
Modern Implants
- Likely improved outcomes compared to older data
Patient Selection
Ideal Candidate
- Good bone quality
- Neutral alignment
- Stable ankle
- Adequate proprioception
- Age >65 years
Common Indications
- Post-traumatic arthritis (most common)
- Inflammatory arthritis (less common now)
Contraindications
Absolute
- Active infection
Relative
- Severe deformity (>20° varus/valgus)
- Neuromuscular instability (e.g., Charcot, cavovarus)
- Severe bone loss or osteoporosis
Preoperative Evaluation
Imaging
X-ray
- Weight-bearing AP and lateral views
CT Scan (Essential)
- Detects:
- Bone defects
- Cysts
- Alignment
Long-Leg Alignment Views
- Assess mechanical axis
- Identify proximal deformities
MRI
- Not routinely required
- Rarely changes management
Surgical Approach
Standard Approach
- Midline anterior approach
Patient Positioning
- Supine
- Leg slightly elevated
Key Surgical Interval
- Between:
- Tibialis anterior
- Extensor hallucis longus (EHL)
Additional Points
- Tourniquet commonly used
- Fluoroscopy essential
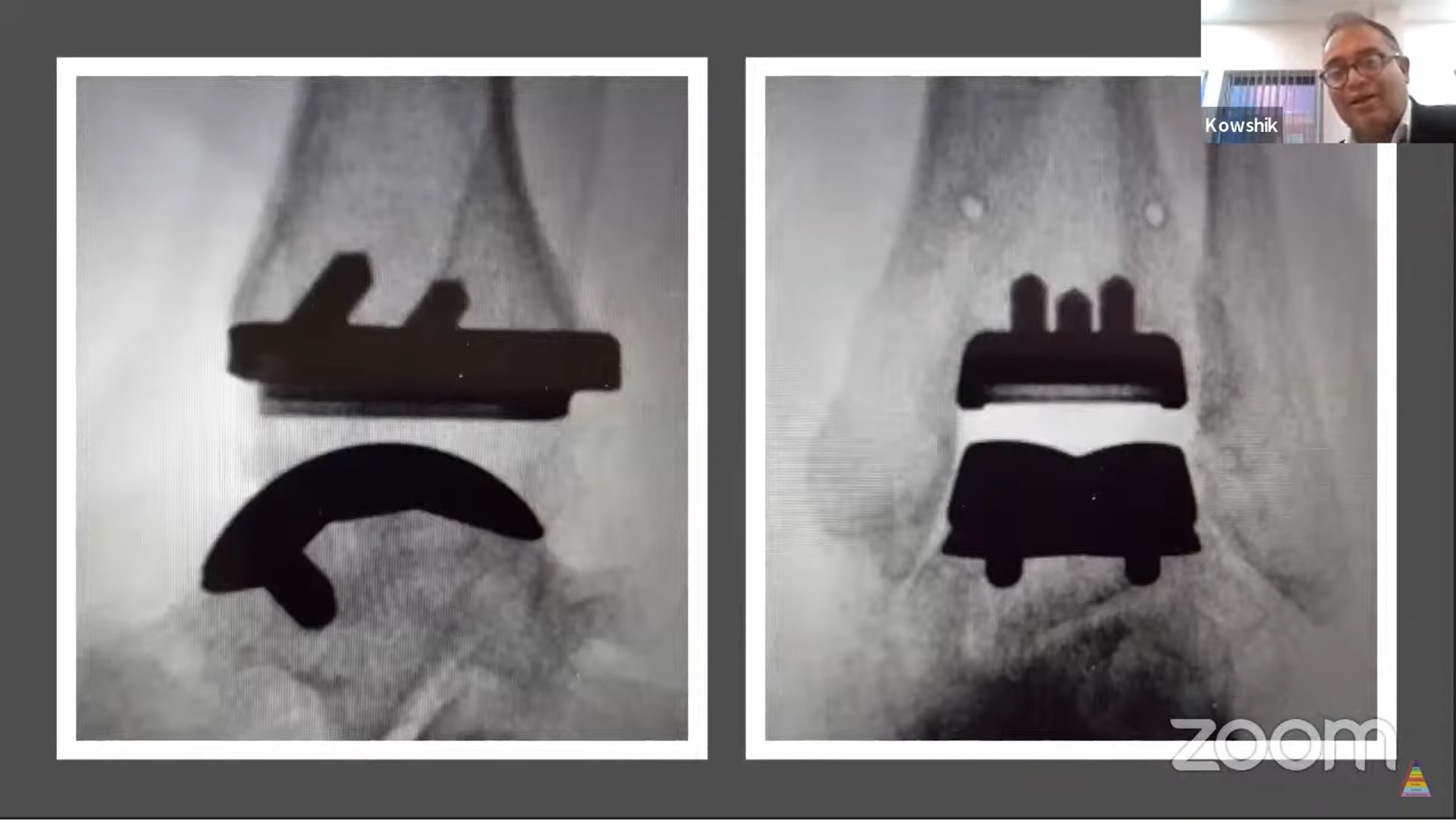
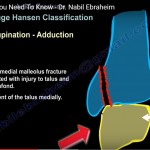
Implantation Technique
Example: Infinity TAR
Design Features
- Porous-coated implant
- Three tibial pegs
- Two talar pegs
- Fixed-bearing polyethylene insert
Advantages
- Accurate implant positioning
- Promotes bone integration
- Minimal gap between bone and implant
Key Surgical Principles
- Sequential bone cuts
- Accurate alignment in:
- AP plane
- Lateral plane
Operative Time
- Approximately 2–3 hours
Management of Deformities (Varus/Valgus)
Key Steps
- Careful patient selection
- Achieve neutral alignment before bone cuts
- Remove osteophytes
- Release soft tissues:
- Deep deltoid ligament
- Posterior tibial tendon (if needed)
- Consider lateral ligament reconstruction
Backup Plan
- Convert to ankle fusion if correction not achievable
Important
- Consent should include possibility of fusion
Concomitant Procedures
May be required in selected cases:
- Achilles tendon lengthening (~20%)
- Calcaneal osteotomy (~10–20%)
- Subtalar or talonavicular fusion (<20%)
- Ligament reconstruction
Key Point
- Most neutral ankles do not require additional procedures
TAR vs Ankle Arthrodesis
Decision Factors
- Patient expectations
- Activity level
- Desire to preserve motion
- Risk of adjacent joint arthritis
General Trend
- Fusion still more common
- TAR usage increasing
Revision Total Ankle Replacement
Revision Risk
- ~8–9% at 10 years
Options
1. Fusion (Most Common)
- Used when bone stock is poor
2. Revision TAR
- Possible in selected patients
- Requires:
- Good tibial and talar bone stock
Challenges
- Bone loss
- Implant loosening
- Technical complexity
Key Takeaways
- TAR is a motion-preserving alternative to ankle fusion
- Requires:
- Careful patient selection
- Precise surgical technique
Advantages
- Better gait mechanics
- Preserved ankle motion
Limitations
- Higher revision rates than hip/knee arthroplasty
- Technically demanding
Clinical Insight
- TAR should be performed in appropriately selected patients by experienced surgeons
Take-Home Message
- TAR is an evolving procedure with improving outcomes
- Not suitable for all patients
- Fusion remains a reliable alternative


Leave a Reply