Courtesy: Prof Nabil Ebraheim, University of Toledo, Ohio, USA
Key Topics Covered
- Lateral malleolus fractures
- Medial malleolus fractures
- Posterior malleolus fractures
- Syndesmotic injuries
- Ankle fractures in diabetic patients
Initial Clinical Assessment
History and Examination
- Mechanism of injury (inversion / eversion)
- Painful, swollen ankle
Differential Diagnosis
Always consider:
- Ligament injuries
- Tendon injuries
- Osteochondral lesions
- Syndesmotic injuries
- Foot fractures
Avoid missing associated injuries
Ottawa Ankle Rules
Indications for X-ray
Perform ankle X-ray if:
- Pain in malleolar zone AND
- Tenderness at posterior edge/tip of malleoli
- Inability to bear weight for 4 steps
Purpose
- Reduce unnecessary imaging
- Improve emergency efficiency
Key Questions in Evaluation
1. Is the fracture displaced or undisplaced?
2. Is the fracture stable or unstable?
These determine management
Undisplaced Ankle Fractures
Definition
- Talar alignment maintained
- Mortise congruent
Key Indicator
Presence of talar shift
Talar Shift
Radiographic Criteria
- Medial clear space > 4 mm
OR - 2 mm greater than superior clear space
Significance
Indicates instability
Stability of Ankle Fractures
Stable Fractures
- Weber A or B
- No medial tenderness
- No medial swelling
Usually low-energy injuries
Important Concept
Medial tenderness – always instability
Why?
- May involve only superficial deltoid ligament
- Deep deltoid may remain intact
Biomechanics of Stability
Deep Deltoid Ligament
- Primary stabilizer
- Prevents lateral talar shift
If Intact
- Talus remains centered
- Fracture may be stable
If Ruptured
- Talar shift occurs
Unstable fracture
Role of Weight-Bearing X-ray
If Deep Deltoid Intact
- Ligament tightens
- Mortise remains congruent
If Ruptured
- Talar shift seen
Confirms instability
Fibular Rotation: Key Insight
- Apparent external rotation may actually be:
- Internal rotation of proximal fibula
If mortise congruent — still undisplaced
Management of Stable Undisplaced Fractures
Example
- Lateral malleolus fracture without medial tenderness
Treatment
- Functional management
- Pain control
- Ankle support
Options
- Ankle brace
- Stirrup splint
- Tubigrip
Weight Bearing
- Full weight bearing allowed
Healing
- ~6 weeks
Follow-Up
- Usually not required
Undisplaced but Potentially Unstable Fractures
Example
- Lateral malleolus fracture with medial tenderness
Concern
- Possible deep deltoid injury
Investigation
Weight-bearing X-ray
Interpretation
Mortise Congruent
- Stable
- Treat conservatively
Talar Shift Present
- Unstable
Requires surgery
Management
- Cast or boot
- Weight bearing as tolerated
- Monitor for displacement
Management of Displaced / Unstable Fractures
General Principle
Most require ORIF
Factors to Consider
- Skin condition
- Swelling / blisters
- Age
- Comorbidities
- Functional demand
Timing of Surgery
- Immediate OR
- Delayed until swelling subsides
Wrinkle Sign
Indicates safe timing for surgery
Fixation Techniques
Lateral Malleolus
Standard Fixation
- One-third tubular plate
- ± Lag screw
Osteoporotic Bone
- Locking plate preferred
Medial Malleolus
Common Features
- Rarely isolated
- Always rule out Maisonneuve fracture
Standard Fixation
- Two cancellous screws
- Often with washers
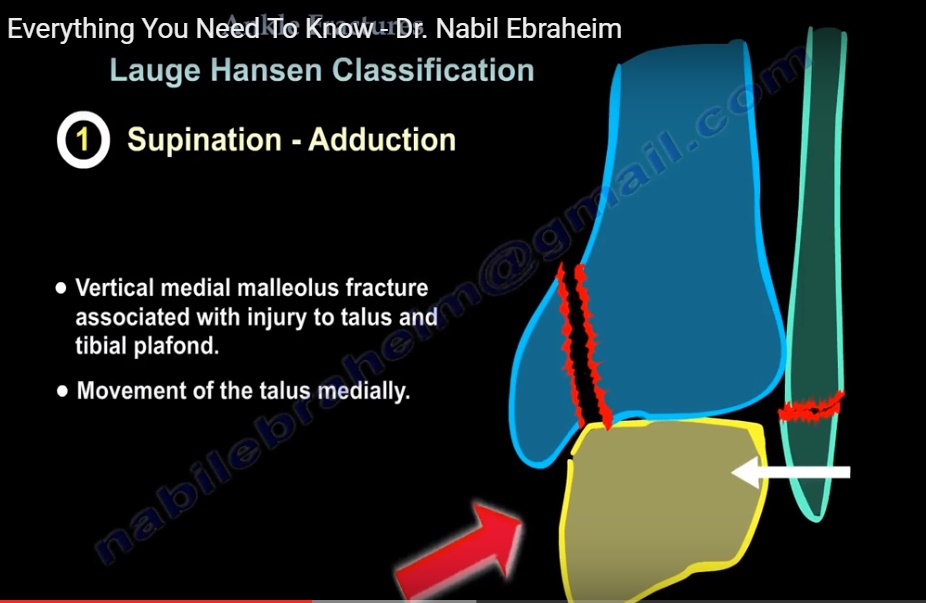
Special Case: Vertical Fracture
- Shear forces present
Preferred Treatment
Buttress plate
Syndesmotic Injuries
Common in
- Weber C fractures
Fixation
- Syndesmotic screw (1.5 cm above joint)
Options
- One or two screws
Weight Bearing
- Usually delayed (~8 weeks)
Screw Removal
- Controversial
Alternative: Tightrope
- Allows micromotion
- No removal required
Posterior Malleolus Fracture
Old Concept
- Fix if >25% articular surface
Modern Concept
Focus on syndesmotic stability, not size
Indications for Fixation
- Displacement > 2 mm
- Syndesmotic instability
- Complex fractures
Preferred Approach
Posterolateral approach
Advantages
- Direct visualization
- Better reduction
- Allows buttress plating
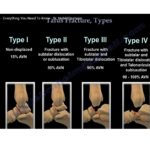
Mason Classification
Type 1
- Small fragment
- Treat with fibular fixation
Type 2A
- Posterolateral fragment
- Plate fixation
Type 2B
- Posteromedial + posterolateral
- Combined fixation
Type 3
- Large pilon-type fragment
- Posteromedial approach
Evidence
- Fixation improves outcomes
- Reduces instability
Ankle Fractures in Diabetic Patients
Key Concern
- Peripheral neuropathy
Risks
- Fixation failure
- Charcot arthropathy
Surgical Strategy
- Strong fixation
- Locking plates
- Additional syndesmotic screws
Postoperative Care
- Prolonged non-weight bearing
- 2–3× longer than normal
Deltoid Ligament Repair
Usually Not Required
Indications
- Persistent talar displacement
- Interposed ligament
- Severe instability
Technique
- Suture anchor repair
Special Techniques in Elderly Patients
Hindfoot Nail
- Allows early weight bearing
Alternative
- Percutaneous Steinmann pin
- Removed after ~12 weeks
Advantages
- Low cost
- Simple technique
Key Take-Home Points
Assessment
- Always evaluate:
- Displacement
- Stability
Critical Indicator
Talar shift = instability
Management
- Stable fractures – conservative
- Unstable fractures – surgical
Modern Insight
- Posterior malleolus fixation depends on stability, not size
Special Populations
- Diabetics require:
- Strong fixation
- Prolonged protection

Leave a Reply