Courtesy: Prof Nabil Ebraheim, University of Toledo, Ohio, USA
Introduction
Pilon fractures involve the distal tibial articular surface (tibial plafond) and are typically caused by high-energy axial loading.
Key Characteristics
- Articular comminution
- Metaphyseal impaction
- Severe soft-tissue injury
Why Classification Matters
- Determines severity
- Guides treatment strategy
- Predicts prognosis
Common Classification Systems
- Rüedi–Allgöwer classification
- AO/OTA classification
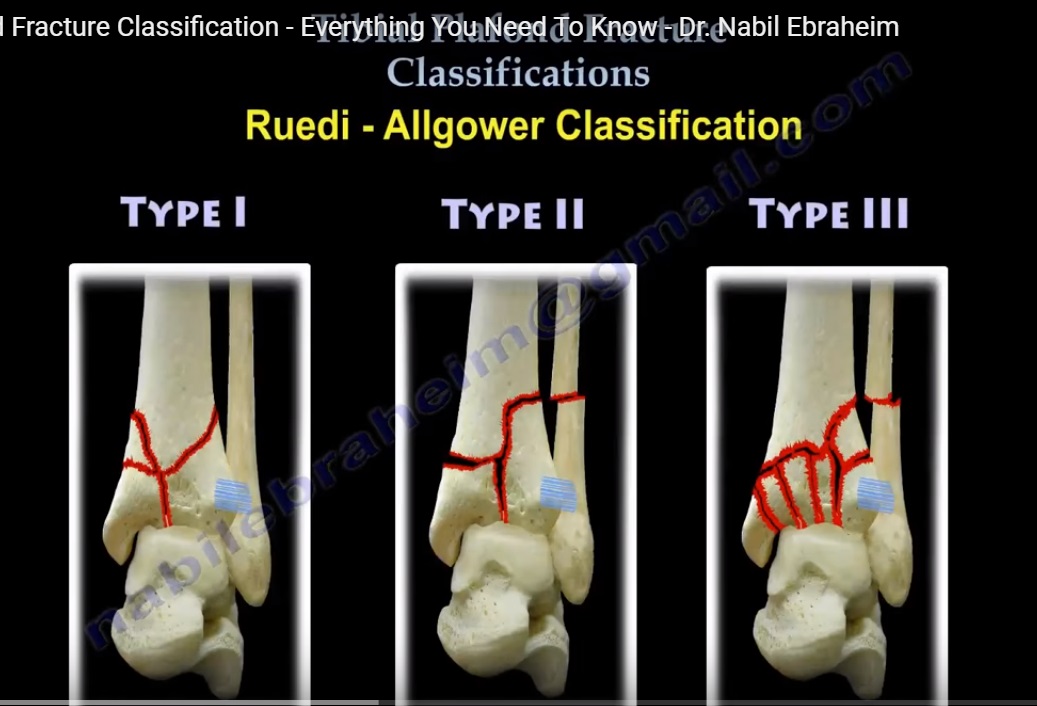
Rüedi–Allgöwer Classification
Concept
Based on:
- Articular displacement
- Degree of comminution
Type I
Features
- Cleavage fracture
- Minimal or no displacement
- Articular surface congruent
- Minimal metaphyseal injury
Prognosis
- Good
Type II
Features
- Displaced intra-articular fracture
- Articular incongruity present
- Minimal metaphyseal comminution
Prognosis
- Moderate
Type III
Features
- Severe articular comminution
- Marked metaphyseal impaction
- Highly unstable
Prognosis
Poor
AO/OTA Classification (Distal Tibia)
Concept
Based on articular involvement
Three Main Types
Type A – Extra-Articular
Features
- No articular involvement
Subtypes
A1
- Simple fracture
A2
- Metaphyseal wedge
A3
- Complex metaphyseal fracture
Type B – Partial Articular
Concept
- Part of articular surface remains attached to shaft
Subtypes
B1 – Split Fracture
- Vertical split of articular surface
B2 – Split + Depression
- Vertical fracture + articular impaction
B3 – Multifragmentary Depression
- Multiple depressed fragments
Type C – Complete Articular
Concept
- Articular surface completely separated from shaft
Subtypes
C1
- Simple articular
- Simple metaphyseal
C2
- Simple articular
- Comminuted metaphyseal
C3
- Multifragmentary articular
- Multifragmentary metaphyseal
Clinical Insight
C3 fractures = most severe injuries
Classical Pilon Fracture Fragments
Three Key Articular Fragments
1. Medial Malleolar Fragment
- Attached to deltoid ligament
2. Chaput Fragment (Anterolateral)
- Attached to AITFL
3. Volkmann Fragment (Posterolateral)
- Attached to PITFL
Clinical Importance
Understanding fragments helps in:
- Surgical planning
- Fixation strategy
Radiological Evaluation
CT Scan (Essential)
Findings
- Articular comminution
- Depressed fragments
- Metaphyseal involvement
- Fragment configuration
Key Role
Mandatory for surgical planning
Surgical Principles
Goals of Treatment
- Restore articular congruity
- Elevate depressed fragments
- Achieve stable fixation
Fixation Methods
- Screws parallel to joint surface
- Buttress plates
- Antiglide plates
Important Clinical Note
Intact Fibula Scenario
If fibula remains intact:
- Force may instead cause:
- Lateral collateral ligament injury
Key Exam Points
High-Yield Facts
- Rüedi Type III – worst prognosis
- AO/OTA C3 – most severe pilon fractures
- CT scan – essential investigation
Classic Fragment Pattern
- Medial
- Chaput
- Volkmann
Clinical Insight
Pilon fractures are:
- High-energy injuries
- Associated with soft-tissue damage
- Require staged management in many cases

Good evening professor Nabil
if we use screws for fixation of type B2 screws should be perpendicular to the fracture line to achieve compression,
thanks prof Nabil,appreciating,very intersting and informative video