Courtesy: FRCS Orth Mentor Group, UK
Overview
Surgical approaches to the shoulder are fundamental in managing:
- Trauma
- Instability
- Degenerative conditions
The two most commonly used approaches are:
- Anterior deltopectoral approach
- Posterior approach
A thorough understanding of anatomy, positioning, and structures at risk is essential for safe and effective surgery.
General Principles for Describing Surgical Approaches
A standardized framework ensures clarity and completeness when describing any surgical approach.
Key Components
- Patient positioning
- Anatomical landmarks
- Intermuscular / internervous plane
- Structures at risk
- Extensibility of the approach
- Technical considerations and pitfalls
Anterior Deltopectoral Approach
Common Indications
- Shoulder arthroplasty
- Anterior shoulder stabilization
- Proximal humerus fracture fixation
- Combined reconstructive procedures
Patient Positioning
- Beach chair position
- Pad placed between the scapulae
- Head securely supported
- Knees slightly flexed (to prevent sliding)
- Ensure access for fluoroscopic imaging
Anatomical Landmarks
- Coracoid process
- Deltopectoral groove
- Lateral border of biceps brachii (for distal extension)
Internervous Plane
The approach utilizes a safe interval between:
- Deltoid muscle
- Innervation: Axillary nerve
- Pectoralis major muscle
- Innervation: Medial and lateral pectoral nerves
This plane allows muscle separation without denervation
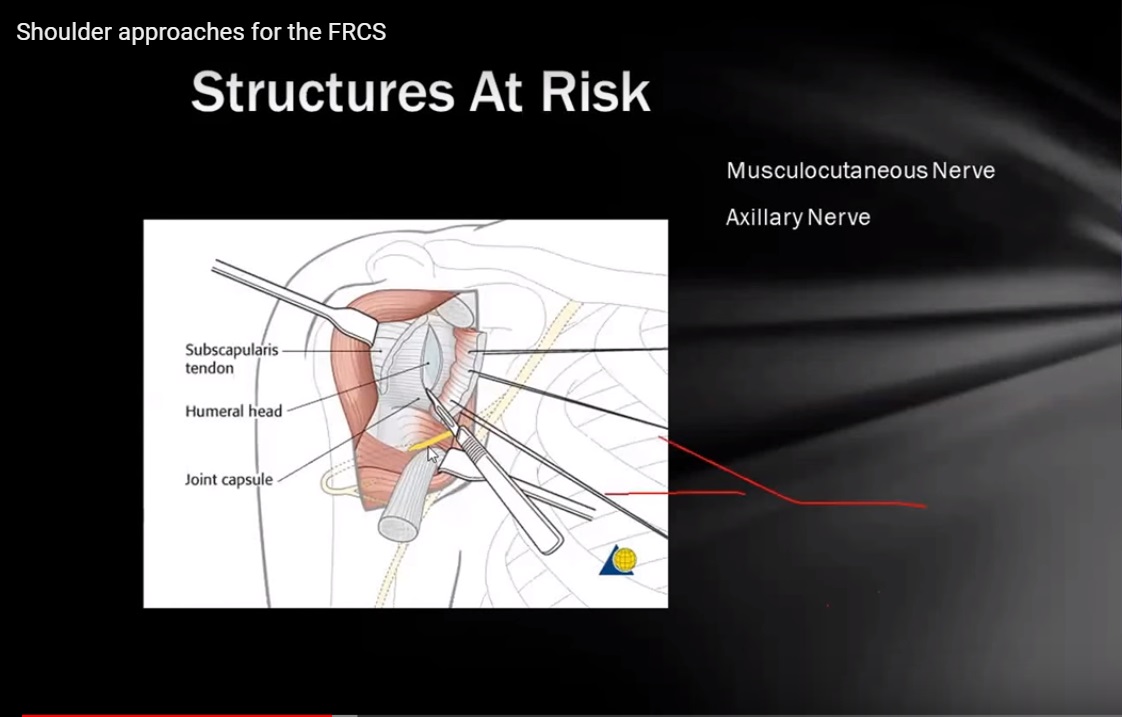
Structures at Risk
Cephalic Vein
- Located within the deltopectoral groove
- Options during surgery:
- Retract medially
- Retract laterally
- Ligate if necessary
Musculocutaneous Nerve
- At risk during mobilization of the conjoint tendon
- Excessive retraction can lead to injury
Axillary Nerve
- Vulnerable during deep dissection
- Risk increases with distal extension of the approach
Key Landmarks in Fracture Fixation
Long Head of Biceps Tendon
- Located in the bicipital groove
- Serves as a guide to identify:
- Greater tuberosity
- Lesser tuberosity
Important Considerations in Trauma
- Avoid dividing the subscapularis tendon
- In proximal humerus fractures:
- Lesser tuberosity remains attached to subscapularis
- Preserving this attachment maintains anatomical alignment
Extension of the Approach
Proximal Extension
- Toward the coracoid process
Distal Extension
- Along the lateral border of the biceps muscle
- Allows exposure of proximal humeral shaft
Precaution: Protect the axillary nerve
Posterior Approach to the Shoulder
Indications
- Posterior shoulder instability
- Posterior capsular procedures
- Fractures involving:
- Posterior glenoid
- Scapula
Patient Positioning
- Lateral decubitus position
- Adequate padding of pressure points
- Proper support of the nonoperative side
- Free positioning of the arm for:
- Manipulation
- Imaging
Anatomical Landmarks
- Acromion
- Spine of the scapula
Incision Options
- Along the scapular spine
- Vertical incision over the posterior shoulder
Internervous Plane
The interval lies between:
- Infraspinatus muscle
- Innervation: Suprascapular nerve
- Teres minor muscle
- Innervation: Axillary nerve
Structures at Risk
Suprascapular Nerve
- Risk during retraction of infraspinatus
Axillary Nerve
- Vulnerable near the quadrangular space
Important Anatomical Spaces in Posterior Shoulder
Understanding these spaces is essential for safe dissection.
Triangular Space
Boundaries
- Superior: Inferior border of teres minor
- Inferior: Superior border of teres major
- Lateral: Long head of triceps
Contents
- Circumflex scapular artery and vein
Quadrangular Space
Boundaries
- Superior: Inferior border of teres minor
- Inferior: Superior border of teres major
- Medial: Long head of triceps
- Lateral: Surgical neck of humerus
Contents
- Axillary nerve
- Posterior circumflex humeral vessels
Clinical Importance:
Key zone for axillary nerve injury
Triangular Interval
Boundaries
- Superior: Inferior border of teres major
- Medial: Long head of triceps
- Lateral: Shaft of humerus
Contents
- Radial nerve
- Profunda brachii artery
Key Points for Describing Surgical Approaches
A structured description improves both learning and clinical application.
Essential Elements
- Patient positioning
- Anatomical landmarks
- Skin incision
- Internervous plane
- Structures at risk
- Possible extensions
- Technical considerations
Take-Home Message
Using a systematic approach ensures:
- Clear understanding
- Safer surgical execution
- Better communication in teaching and exams


Leave a Reply