Courtesy: Prof Nabil Ebraheim, University of Toledo, Ohio, USA
Overview
Selection of the surgical approach in acetabular fractures depends on multiple factors:
Key Determinants
- Location of the fracture within the acetabulum
- Fracture pattern and classification
- Degree of displacement
- Complexity of fracture fragments
Principle
An appropriate approach should:
- Provide adequate exposure for reduction and fixation
- Minimize soft tissue damage and complications
Posterior Approach
Indications
The posterior approach is preferred for fractures involving posterior acetabular structures:
- Posterior wall fractures
- Posterior column fractures
- Combined posterior wall + posterior column fractures
- Posterior wall fractures with transverse patterns
- Selected low transverse fractures
Surgical Considerations
- Provides excellent visualization of posterior structures
- Can be extended with:
- Anterior approach
- Trochanteric osteotomy
Sliding Trochanteric Osteotomy
- Enhances exposure of:
- Acetabular dome
- Superior joint surface
Complications
1. Sciatic Nerve Injury
- Requires meticulous protection during dissection
2. Limited Anterior Exposure
- Anteriorly displaced fractures may not be adequately visualized
3. Femoral Head Vascular Compromise
- Avoid excessive capsular damage
- Preserve ~1 cm capsular cuff
Sciatic Nerve Protection
- Keep the knee flexed to reduce tension
- Especially important during traction
Retractor Placement
- Retractor may be placed in the greater sciatic notch
- Obturator internus muscle acts as a protective buffer
Anatomical Relationships
- Sciatic nerve lies:
- Posterior to obturator internus
- Anterior to piriformis
Anterior Approach
Indications
Used for fractures involving anterior acetabular structures:
- Anterior wall fractures
- Anterior column fractures
- Both column fractures
- High transverse fractures
- Associated anterior column + posterior hemi-transverse fractures
Surgical Windows
The anterior approach typically involves three windows:
1. Medial Window
Contents
- Spermatic cord (male) / round ligament (female)
- Ilioinguinal nerve
Risk
- Inadequate closure ? postoperative hernia
2. Middle Window
Contents
- External iliac vessels
- Corona mortis (variable vascular connection)
3. Lateral Window
Contents
- Iliopsoas muscle
- Femoral nerve
- Lateral femoral cutaneous nerve
Important
- All structures must be carefully protected
Iliopectineal Fascia
Anatomy
- Lies between middle and lateral windows
Surgical Step
- Incision along the pelvic brim
Benefit
- Improves communication between:
- True pelvis
- False pelvis
- Enhances visualization and reduction
Important Risks
1. Lateral Femoral Cutaneous Nerve Injury
- Leads to sensory disturbance over lateral thigh
2. Abdominal Wall Hernia
- Due to improper muscle closure
3. Corona Mortis Injury
Characteristics
- Vascular connection between:
- Internal iliac system
- External iliac / inferior epigastric vessels
- Located on superior pubic ramus
- Typically 3–7 cm from pubic symphysis
Clinical Significance
- Injury can cause severe, difficult-to-control bleeding
Management of Transverse Fractures
- High transverse fractures ? Usually anterior approach
- Low transverse fractures ? May be treated via posterior approach
Combined Surgical Approaches
Indications
Used for complex fracture patterns involving both columns:
- T-shaped fractures
- Combined anterior and posterior injuries
Rationale
- Allows complete visualization and reduction of both components
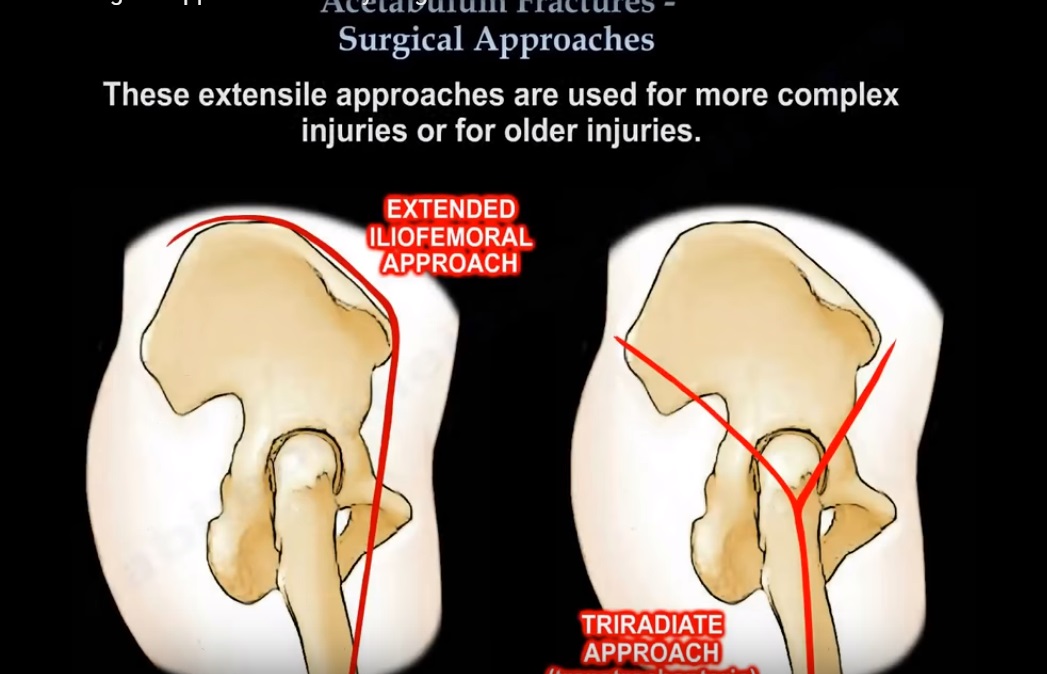
Extended Surgical Approaches
Types
- Extended iliofemoral approach
- Triradiate trans-trochanteric approach
Indications
- Severe or highly complex fractures
- Need for extensive visualization of:
- Both columns
- Acetabular dome
Complications
1. Gluteal Muscle Necrosis
- Due to compromised blood supply
2. Heterotopic Ossification (HO)
- Increased risk with extensive dissection
Muscle Consideration
- Gluteus medius and minimus remain attached mainly via:
- Superior gluteal vessel pedicle
Heterotopic Ossification (HO)
Risk
- Higher in extended approaches
Prevention Strategies
- Low-dose radiation therapy (within 72 hours post-op)
- Indomethacin therapy (~6 weeks)
Complete prevention is not always possible
Preference for Dual Approaches
Many surgeons prefer separate anterior and posterior approaches over extended approaches.
Advantages
- Reduced soft tissue damage
- Lower risk of heterotopic ossification
- Better control of individual fracture fragments
Safe Screw Placement
Concern
- Certain regions of acetabulum are danger zones
Risk
- Intra-articular screw penetration
Precautions
- Use multiple fluoroscopic views
- Consider direct visualization
Fixation of Posterior Wall Fractures
Techniques
- Buttress plates
- Hook plates
Special Situation: Marginal Impaction
- Elevate impacted fragment
- Fill defect with bone graft
Soft Tissue Injuries in Acetabular Trauma
Morel-Lavallée Lesion
Definition
- Closed degloving injury
- Separation of:
- Skin and subcutaneous tissue
- From underlying fascia
Common Locations
- Pelvis
- Greater trochanter region
Clinical Importance
- Frequently associated with high-energy trauma
Surgical Concern
- Increased risk of infection
- Up to 30% of operative sites may be colonized
Key Takeaways
- Approach selection is fracture-specific
- Posterior– posterior structures
- Anterior– anterior structures
- Complex fractures — may require combined or extended approaches
- Careful handling of:
- Neurovascular structures
- Soft tissues
- Screw placement
Leave a Reply