Courtesy: FRCS Orth Mentor Group, UK
Overview
- Surgical approaches to the shoulder are essential for treating trauma, instability, and degenerative conditions.
- Two commonly discussed approaches are:
- The anterior deltopectoral approach
- The posterior approach
- Understanding anatomy, patient positioning, and structures at risk is crucial for safe and effective surgery.
General Principles for Describing Any Surgical Approach
When explaining a surgical approach, several key components should always be addressed:
- Patient positioning
- Anatomical landmarks
- Intermuscular or internervous plane
- Structures at risk
- Extent of the approach (limited or extensile)
- Technical considerations and potential pitfalls
These principles provide a structured way to describe any surgical approach and ensure that all important aspects are covered.
Anterior Deltopectoral Approach
Common Indications
- Shoulder arthroplasty procedures
- Anterior shoulder stabilization
- Fixation of proximal humerus fractures
- Combined reconstructive procedures
Patient Positioning
- The patient is positioned in the beach chair position.
- A support pad is placed between the scapulae.
- The head is secured properly.
- Knees are slightly flexed to prevent sliding during the procedure.
- The operative field should allow access for fluoroscopic imaging when required.
Anatomical Landmarks
Important landmarks used to guide the incision include:
- Coracoid process
- Deltopectoral groove
- Lateral border of the biceps brachii (when extension of the approach is required)
Internervous Plane
The surgical interval is located between:
- Deltoid muscle
- Innervation: Axillary nerve
- Pectoralis major muscle
- Innervation: Medial and lateral pectoral nerves
This internervous plane allows safe separation of muscles without compromising their nerve supply.
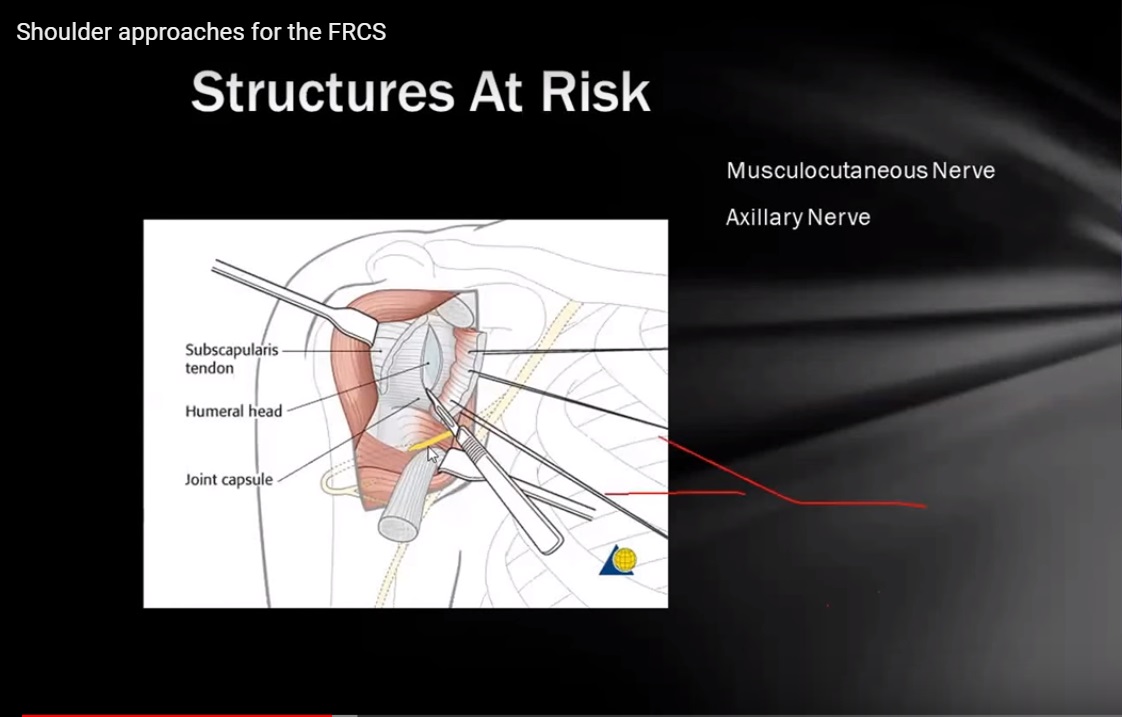
Structures at Risk
Cephalic Vein
- Located in the deltopectoral groove.
- It may be:
- Retracted medially
- Retracted laterally
- Occasionally ligated if severely traumatized during retraction.
Musculocutaneous Nerve
- At risk particularly when the conjoint tendon is mobilized.
- Excessive retraction may cause nerve injury.
Axillary Nerve
- Important to protect during deeper dissection.
- Injury can occur during excessive retraction or when extending the approach distally.
Key Surgical Landmarks During Fracture Fixation
- Identification of the long head of the biceps tendon is essential.
- The tendon lies within the bicipital groove and helps identify:
- Greater tuberosity
- Lesser tuberosity
Important Considerations in Trauma
- The subscapularis tendon should not be divided during fracture surgery.
- In proximal humerus fractures, the lesser tuberosity remains attached to the subscapularis, and preserving this structure helps maintain anatomical integrity.
Extension of the Approach
The incision can be extended when necessary:
- Proximally toward the coracoid process.
- Distally along the lateral border of the biceps muscle to expose the proximal humeral shaft.
Care must be taken to protect the axillary nerve during distal extension.
Posterior Approach to the Shoulder
Indications
- Posterior shoulder instability
- Posterior capsular procedures
- Certain fractures involving the posterior glenoid or scapula
Although less frequently used in routine practice, this approach is important due to its anatomical relevance.
Patient Positioning
- The patient is placed in the lateral decubitus position.
- Adequate padding is required to protect pressure points.
- The nonoperative side must be carefully supported.
- The arm should be positioned freely to allow manipulation and imaging if necessary.
Anatomical Landmarks
Key landmarks include:
- Acromion
- Spine of the scapula
The incision may run:
- Along the scapular spine, or
- Vertically over the posterior shoulder depending on the surgical objective.
Internervous Plane
The interval lies between:
- Infraspinatus muscle
- Innervation: Suprascapular nerve
- Teres minor muscle
- Innervation: Axillary nerve
This plane allows safe entry to the posterior shoulder structures.
Structures at Risk
Suprascapular Nerve
- Can be injured by excessive retraction of the infraspinatus muscle.
Axillary Nerve
- Vulnerable near the quadrangular space.
Important Anatomical Spaces Around the Posterior Shoulder
Understanding the spaces around the posterior shoulder is critical when using this approach.
Triangular Space
Boundaries
- Superior: Inferior border of teres minor
- Inferior: Superior border of teres major
- Lateral: Long head of the triceps
Contents
- Circumflex scapular artery and vein
Quadrangular Space
Boundaries
- Superior: Inferior border of teres minor
- Inferior: Superior border of teres major
- Medial: Long head of the triceps
- Lateral: Surgical neck of the humerus
Contents
- Axillary nerve
- Posterior circumflex humeral artery and vein
This space is particularly important during posterior surgical exposure because the axillary nerve passes through it.
Triangular Interval
Boundaries
- Superior: Inferior border of teres major
- Medial: Long head of the triceps
- Lateral: Shaft of the humerus
Contents
- Radial nerve
- Profunda brachii artery
This interval is relevant during surgical approaches to the posterior humeral shaft.
Key Points for Surgical Approach Descriptions
A systematic explanation of surgical approaches improves clarity and completeness.
Essential points to include are:
- Patient positioning
- Surgical landmarks
- Skin incision
- Internervous plane
- Structures at risk
- Possible extensions of the approach
- Technical considerations
Following this structured method ensures that the description remains concise and clinically relevant.


Leave a Reply