Courtesy – Dr Sanjeev Madan, Dr Ashok Shyam, Ortho TV
Slipped Capital Femoral Epiphysis (SCFE)
Introduction
Slipped capital femoral epiphysis (SCFE) is one of the most common hip disorders in adolescents.
Despite its name, SCFE is technically a misnomer because:
- The femoral head remains within the acetabulum
- The metaphysis and femoral shaft displace relative to the epiphysis
The displacement typically occurs:
- Inferiorly
- Posteriorly
Early diagnosis is essential to prevent long-term complications such as:
- Avascular necrosis
- Femoroacetabular impingement
- Early osteoarthritis
Epidemiology
Age Group
SCFE most commonly occurs between:
- 8–15 years of age
during the adolescent growth spurt.
Gender Distribution
The condition is more common in:
- Boys than girls
with an approximate ratio of:
- 1.5:1
Incidence
Reported incidence is approximately:
- 10.8 per 100,000 children
Bilateral Involvement
Bilateral disease occurs in:
- Approximately 20% of symptomatic patients
The true incidence is higher when asymptomatic slips are included.
Pathophysiology
Basic Mechanism
SCFE occurs through weakness of the:
- Proximal femoral physis
The femoral neck and shaft move relative to the stable epiphysis.
Direction of Slip
The metaphysis typically displaces:
- Anteriorly
- Superiorly
relative to the femoral head, producing an apparent:
- Posterior and inferior slip of the epiphysis
Resulting Deformity
This leads to:
- External rotation deformity
- Loss of internal rotation
- Altered hip mechanics
Etiology and Risk Factors
Mechanical and Biological Factors
The adolescent growth plate becomes vulnerable during rapid growth.
Contributing factors include:
- Physeal weakness
- Mechanical loading
- Hormonal influences
Obesity
Obesity is one of the strongest risk factors because it increases:
- Shear forces across the physis
Endocrine Disorders
SCFE may be associated with:
- Hypothyroidism
- Growth hormone abnormalities
- Hypogonadism
Other Associated Conditions
Additional associations include:
- Renal osteodystrophy
- Genetic predisposition
Atypical SCFE in younger children or thin adolescents should prompt endocrine evaluation.
Clinical Presentation
Pain
Patients commonly present with:
- Hip pain
- Groin pain
- Thigh pain
Importantly, pain may be referred to the:
- Knee
which may delay diagnosis.
Limp
A limp is a frequent presenting complaint.
Range of Motion
Characteristic findings include:
- Reduced internal rotation
- Loss of hip flexion
- Obligatory external rotation during hip flexion
Important Clinical Pearl
Always examine the hip in adolescents presenting with:
- Unexplained knee pain
Classification
Stable vs Unstable SCFE
Stable SCFE
The patient can:
- Bear weight, even with crutches
Stable slips generally have a better prognosis.
Unstable SCFE
The patient is:
- Unable to bear weight
Unstable slips carry a significantly higher risk of:
- Avascular Necrosis
Acute vs Chronic
SCFE may also be classified as:
- Acute
- Chronic
- Acute-on-chronic
based on symptom duration.
Severity Classification
Severity is commonly determined using:
- Southwick angle
and categorized as:
- Mild
- Moderate
- Severe
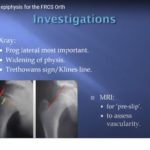
Imaging
Plain Radiographs
Standard imaging includes:
- AP pelvis radiograph
- Frog-leg lateral view
The lateral view is particularly useful for detecting subtle slips.
Klein’s Line
Klein’s line is drawn along the superior femoral neck.
In normal hips:
- The line intersects the femoral head
In SCFE:
- The line fails to intersect the epiphysis
This is an important radiographic sign.
Southwick Angle
The Southwick angle measures:
- Degree of slip severity
A significantly increased angle indicates more severe deformity.
Differential Diagnosis
Conditions that may mimic SCFE include:
- Perthes Disease
- Hip infection
- Transient synovitis
- Femoral neck fracture
- Tumors
Management Principles
Goal of Treatment
The primary goal is to:
- Prevent further slip progression
while preserving:
- Femoral head vascularity
In-Situ Pinning
Gold Standard Treatment
The standard treatment for most stable slips is:
- In-situ screw fixation
This stabilizes the physis without attempting forceful reduction.
Surgical Technique Principles
Important considerations include:
- Accurate screw positioning
- Adequate thread purchase across the physis
- Avoiding joint penetration
Contralateral Hip Monitoring
Because bilateral involvement is common:
- The opposite hip should be monitored carefully
Prophylactic fixation may be considered in selected high-risk patients.
Complications
Avascular Necrosis
AVN is one of the most serious complications, especially in:
- Unstable SCFE
Femoroacetabular Impingement
Residual deformity may produce:
- Cam-type impingement
leading to cartilage damage and early arthritis.
Chondrolysis
Rarely, patients may develop:
- Rapid cartilage loss
- Severe stiffness
Long-Term Degeneration
Residual deformity increases the risk of:
- Early osteoarthritis
Prognostic Factors
Better Prognosis
Associated with:
- Early diagnosis
- Stable slips
- Mild deformity
Worse Prognosis
Associated with:
- Delayed diagnosis
- Severe slip
- Unstable SCFE
- AVN
Follow-Up
Long-term follow-up is important to evaluate for:
- Slip progression
- Contralateral involvement
- Impingement
- Degenerative changes
Key Clinical Pearls
- SCFE is the most common adolescent hip disorder.
- Knee pain may be the presenting symptom.
- Loss of internal rotation is a key clinical finding.
- Frog-leg lateral radiographs are extremely important.
- Klein’s line helps identify subtle slips.
- Stable slips have a much better prognosis than unstable slips.
- In-situ pinning is the standard treatment.
- Early diagnosis reduces long-term complications.
Final Take-Home Message
Slipped capital femoral epiphysis is a growth plate disorder of adolescence caused by displacement of the proximal femoral metaphysis relative to the epiphysis.
The condition commonly presents with:
- Limp
- Hip pain
- Referred knee pain
Early recognition and prompt stabilization are essential to prevent serious complications such as avascular necrosis and femoroacetabular impingement.
Any adolescent with unexplained knee pain or limp should always undergo careful hip evaluation.



Leave a Reply