Courtesy: Amr Abdelgawad, Maimonaides Medical Centre, Brooklyn, New York, USA
Slipped Capital Femoral Epiphysis (SCFE)
Introduction
Slipped capital femoral epiphysis (SCFE) is one of the most common hip disorders affecting adolescents.
It involves:
- Displacement of the proximal femoral metaphysis relative to the epiphysis
Importantly, the femoral head remains within the acetabulum, making the term “slipped epiphysis” technically a misnomer.
Basic Pathology
Normal Hip Relationship
The normal proximal femur is often described as:
- “Ice cream on a cone”
where:
- The epiphysis represents the ice cream
- The metaphysis and neck represent the cone
Pathological Mechanism in SCFE
In SCFE:
- The metaphysis and femoral neck displace
- The epiphysis remains relatively stable within the acetabulum
This produces:
- Posterior and inferior displacement of the epiphysis relative to the neck
Epidemiology
Typical Patient Profile
SCFE commonly affects:
- Overweight adolescents
and is more common in:
- Boys
Age Group
Typical age at presentation:
- Girls: approximately 11 years
- Boys: approximately 13 years
Bilateral Involvement
Bilateral disease occurs in approximately:
- 50% of patients
Among these:
- One-third present simultaneously
- Two-thirds develop contralateral involvement later
Because of this, both hips must always be evaluated.
Etiology and Risk Factors
Idiopathic SCFE
Most cases are:
- Idiopathic
and occur during periods of rapid growth.
Endocrine Disorders
Associated endocrine abnormalities include:
- Hypothyroidism
- Growth hormone disorders
Other Associated Conditions
Additional causes and associations include:
- Renal osteodystrophy
- Trauma
Atypical presentations should prompt further metabolic or endocrine evaluation.
Clinical Presentation
Pain
Patients may present with:
- Hip pain
- Groin pain
- Thigh pain
Importantly, isolated:
- Knee pain
may be the presenting symptom and can delay diagnosis.
Limp
Children frequently present with:
- Limping
- External rotation gait
Hip Examination Findings
Characteristic examination findings include:
- Reduced internal rotation
- Obligatory external rotation during hip flexion
Loss of internal rotation is a key clinical clue.
Classification
Stability Classification
This is the most clinically important classification because it predicts the risk of complications.
Stable SCFE
The patient:
- Can bear weight, with or without crutches
Stable slips have:
- Lower risk of avascular necrosis
Unstable SCFE
The patient:
- Cannot bear weight
Unstable SCFE carries a significantly higher risk of:
- Avascular Necrosis
Duration-Based Classification
Acute SCFE
- Symptoms present for less than 3 weeks
Chronic SCFE
- Symptoms present for more than 3 weeks
Acute-on-Chronic SCFE
- Chronic symptoms with sudden worsening
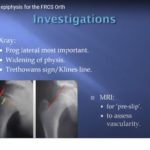
Imaging
Standard Radiographs
Essential imaging includes:
- AP pelvis radiograph
- Frog-leg lateral radiograph
The frog-leg lateral view is especially useful for detecting subtle slips.
Radiographic Findings
Common findings include:
- Metaphyseal displacement
- Widened physis
- Loss of normal femoral head-neck alignment
Klein’s Line
Klein’s line is drawn along the superior border of the femoral neck.
Normal Hip
- The line intersects the femoral epiphysis
SCFE
- The line fails to intersect the epiphysis
This is an important diagnostic sign.
Other Radiographic Signs
Additional findings may include:
- Crescent sign
- Physeal widening
especially in early disease.
Management
Initial Emergency Management
All suspected SCFE patients should immediately be:
- Made non-weight bearing
- Referred urgently to orthopedics
Definitive Treatment
In-Situ Pinning
The gold standard treatment is:
- In-situ fixation using a single screw
The aim is to:
- Prevent further slipping
- Stabilize the physis
Surgical Principles
Important principles include:
- Avoid aggressive reduction
- Preserve femoral head blood supply
- Ensure appropriate screw placement
Management of Unstable SCFE
In unstable slips:
- Gentle reduction may be performed if necessary
- Fixation is then carried out carefully
Forceful reduction should be avoided because it increases AVN risk.
Endocrine Evaluation
Endocrine workup is generally reserved for:
- Atypical presentations
- Younger children
- Thin patients
- Bilateral severe disease
Complications
Avascular Necrosis
AVN is the most feared complication, especially in:
- Unstable SCFE
Residual Deformity
Persistent deformity may result in:
- Femoroacetabular impingement
- Limited hip motion
Osteoarthritis
Long-term deformity can lead to:
- Early degenerative arthritis
Follow-Up
Long-term follow-up is important to monitor for:
- Contralateral slip
- Growth disturbances
- Residual deformity
- Degenerative changes
Key Clinical Pearls
- SCFE is a disorder of adolescent growth plates.
- The epiphysis remains within the acetabulum.
- Knee pain may be the presenting complaint.
- Loss of internal rotation is an important examination finding.
- Frog-leg lateral radiographs are essential.
- Klein’s line helps detect subtle slips.
- Stability classification predicts AVN risk.
- In-situ pinning is the standard treatment.
- Early diagnosis significantly improves outcomes.
Final Take-Home Message
Slipped capital femoral epiphysis is a common adolescent hip disorder caused by displacement through the proximal femoral physis.
Any adolescent presenting with:
- Limp
- Hip pain
- Unexplained knee pain
should undergo careful hip evaluation.
Prompt diagnosis and early stabilization are essential to prevent serious complications such as avascular necrosis, deformity, and early osteoarthritis.



Leave a Reply