Courtesy: Prof Nabil Ebraheim, University of Toledo, Ohio, USA
-
Shoulder Dislocation: Associated Lesions, Diagnosis, and Clinical Pearls
Introduction
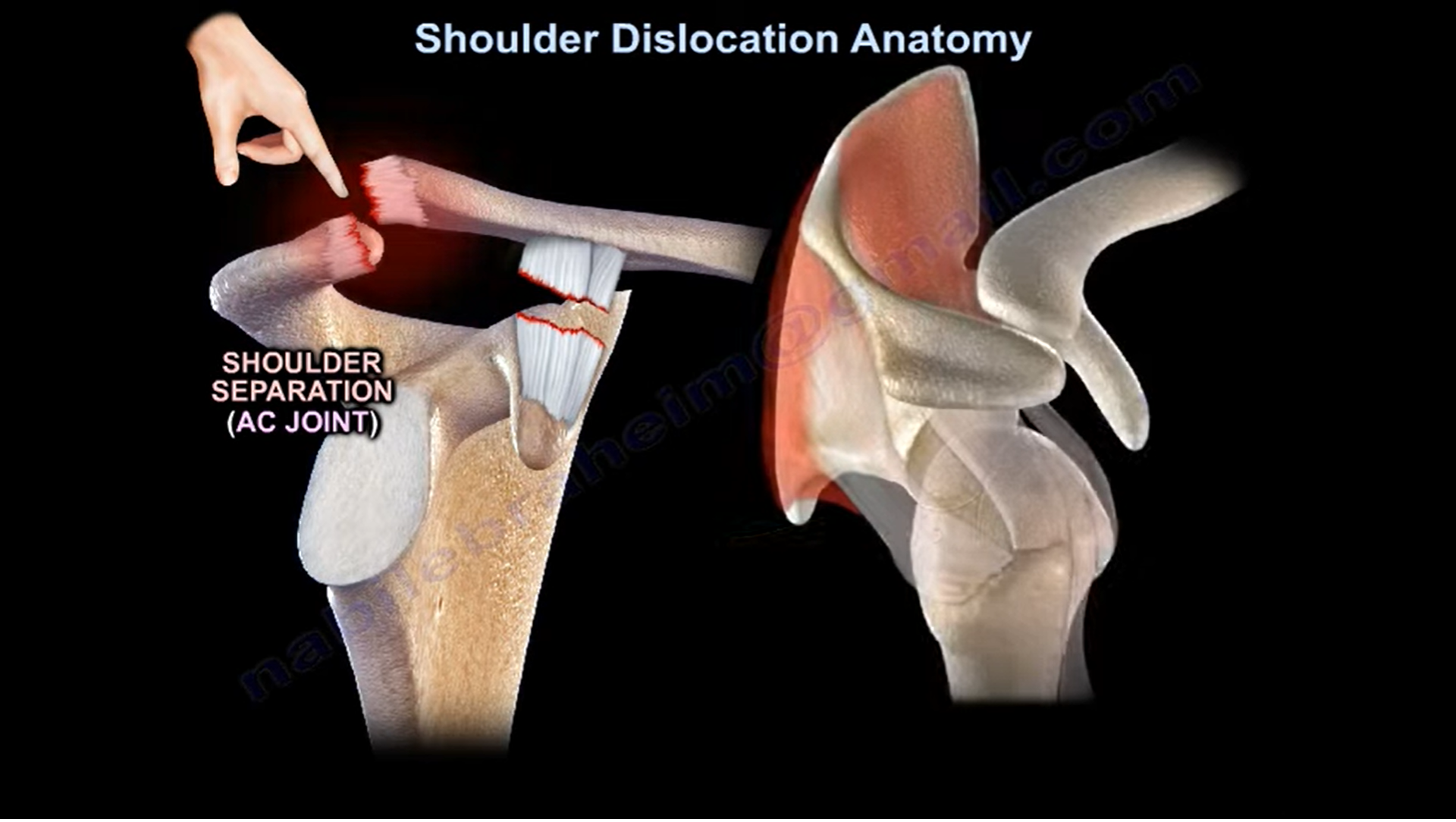
Shoulder dislocation refers to displacement of the humeral head from the glenoid cavity of the scapula. It is important to distinguish a shoulder dislocation from an acromioclavicular (AC) joint injury.
Shoulder Dislocation vs Shoulder Separation
Shoulder Dislocation
- Dislocation of the humeral head from the glenoid.
- Involves the glenohumeral joint.
Shoulder Separation
- Injury to the acromioclavicular (AC) joint.
- Does not involve dislocation of the glenohumeral joint.
Common Associated Lesions in Shoulder Dislocation
The most common injuries associated with shoulder dislocation include:
- Bankart lesion
- Hill-Sachs lesion
- Rotator cuff tear (especially in elderly patients)
- Axillary nerve injury
- Greater tuberosity fracture
- Lesser tuberosity fracture
Anatomy of the Glenoid Labrum
The shoulder joint is formed by the articulation between the humeral head and the glenoid.
The glenoid labrum is a fibrocartilaginous structure attached to the rim of the glenoid.
Functions of the Labrum
- Deepens the glenoid socket by approximately 50%
- Increases joint stability
- Acts as a bumper within the joint capsule
- Provides attachment for capsuloligamentous structures
Bankart Lesion
Definition
A Bankart lesion is an avulsion of the anteroinferior labrum and the anterior band of the inferior glenohumeral ligament from the anterior inferior glenoid.
It occurs as a result of anterior shoulder dislocation.
Clinical Importance
- Strongly associated with recurrent shoulder instability
- Particularly common in young patients
- Present in approximately 80% to 90% of patients with traumatic anterior instability
TUBS Lesion
The classic acronym TUBS stands for:
- Traumatic
- Unilateral
- Bankart lesion
- Surgery often required
Types of Bankart Lesions
Soft Tissue Bankart
- Pure labral avulsion
- No associated fracture
Bony Bankart
- Associated fracture of the anterior glenoid rim
- Seen in approximately 50% of recurrent dislocations
Glenoid Bone Loss
Significant glenoid bone deficiency greatly increases instability.
Critical Bone Loss
When glenoid bone loss exceeds approximately 20% to 25%:
- Soft tissue repair alone has a high failure rate
- Arthroscopic Bankart repair may not be sufficient
- Bony reconstruction procedures are often required
Evaluation of Glenoid Bone Loss
Best Imaging Study
CT scan with three dimensional reconstruction
This provides the most accurate assessment of:
- Glenoid morphology
- Percentage of bone loss
- Surgical planning
Surgical Management
Latarjet Procedure
Indications:
- Glenoid bone loss greater than 20% to 25%
- Inverted pear glenoid deformity
- Failed previous stabilization procedures
Technique:
- Transfer of the coracoid process to the anterior glenoid
Benefits:
- Restores glenoid bone stock
- Provides dynamic sling effect
- Reduces recurrence rates
Alternative Options
- Iliac crest bone grafting
Rotator Cuff Tears After Shoulder Dislocation
Rotator cuff tears become increasingly common with advancing age.
Incidence
- Approximately 30% in patients older than 40 years
- Up to 80% in patients older than 60 years
Clinical Pearl
If a patient cannot actively elevate the arm after reduction:
Young Patient
Think:
- Axillary nerve palsy
Elderly Patient
Think:
- Rotator cuff tear
Hill-Sachs Lesion
Definition
A Hill-Sachs lesion is a compression fracture of the posterolateral humeral head caused by impaction against the anterior inferior glenoid rim during anterior shoulder dislocation.
Incidence
- Present in approximately 80% of acute traumatic dislocations
- Present in approximately 25% of traumatic subluxations
Management
Remplissage Procedure
Indications:
- Large Hill-Sachs defects
- Typically greater than 25% of the humeral head
Technique:
- Posterior capsule and infraspinatus tendon are sutured into the defect
Purpose:
- Converts the defect into an extra-articular lesion
- Reduces engagement and recurrent instability
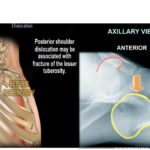
Posterior Shoulder Dislocation
Associated Injuries
Posterior shoulder dislocations may be associated with:
- Reverse Hill-Sachs lesion
- Lesser tuberosity fractures
McLaughlin Procedure
Indications:
- Posterior dislocation less than six months old
- Reverse Hill-Sachs lesion involving less than 40% of the humeral head
Technique:
- Transfer of the subscapularis tendon into the defect
- May include transfer of the lesser tuberosity with attached subscapularis
HAGL Lesion
Definition
HAGL stands for:
Humeral Avulsion of the Glenohumeral Ligament
Specifically involving the inferior glenohumeral ligament.
Characteristics
- Uncommon injury
- Frequently missed
- Common in violent sports injuries
- Can cause recurrent instability
MRI Findings
- Irregularity of the inferior capsular pouch
- Disruption of the inferior glenohumeral ligament attachment
Clinical Importance
Failure to recognize and repair a HAGL lesion is associated with a high recurrence rate.
Inferior Glenohumeral Ligament Complex
Anterior Inferior Glenohumeral Ligament
Primary restraint to anterior translation when the shoulder is:
- Abducted 90 degrees
- Externally rotated
This is the classic apprehension position.
Posterior Inferior Glenohumeral Ligament
Primary restraint to posterior translation when the shoulder is:
- Flexed 90 degrees
- Internally rotated
Labral Tears and Shoulder Instability
Anterior Labral Tears
Clinical Features
- Anterior instability
- Recurrent dislocations
MRI
- Best visualized on axial images
- MR arthrography improves detection
Clinical Test
- Apprehension test
Posterior Labral Tears
Clinical Features
- Posterior instability
- Often causes pain more than instability
MRI
- Best seen on axial images
Clinical Tests
- Jerk test
- Kim test
Why Are Posterior Dislocations Common After Seizures and Electric Shock?
During seizures and electric shock injuries:
- Internal rotators contract violently
- Internal rotators are stronger than external rotators
Major internal rotators include:
- Subscapularis
- Latissimus dorsi
- Pectoralis major
The resulting force drives the humeral head posteriorly, producing posterior shoulder dislocation.
Normal Variants of the Labrum
Certain anatomical variants can mimic labral tears on MRI.
Sublabral Foramen
A normal detachment of the superior labrum from the glenoid.
Buford Complex
Characterized by:
- Absent anterosuperior labrum
- Thick middle glenohumeral ligament
Clinical Pearl
These are normal anatomical variants and should not be repaired.
Inappropriate repair may result in:
- Loss of shoulder motion
- Significant loss of external rotation
- Persistent postoperative stiffness
Key Takeaways
- Shoulder dislocation is different from AC joint separation.
- Bankart lesions are the most common soft tissue injury after anterior shoulder dislocation.
- Glenoid bone loss greater than 20% to 25% often requires bony augmentation procedures such as the Latarjet procedure.
- Hill-Sachs lesions occur due to impaction of the humeral head against the glenoid.
- Rotator cuff tears are common in elderly patients after dislocation.
- Axillary nerve injury should be suspected in younger patients unable to elevate the arm after reduction.
- HAGL lesions are uncommon but important causes of recurrent instability.
- Posterior shoulder dislocations are classically associated with seizures and electric shock injuries.
- Sublabral foramen and Buford complex are normal variants and should not be mistaken for labral tears.


Leave a Reply