Background
-
In 1983, Charles Neer, Craig, and Fukuda described cuff tear arthropathy as a distinct clinical entity.
-
It represents a form of degenerative arthritis associated with long-standing, massive rotator cuff tears.
-
Loss of rotator cuff function results in superior migration of the humeral head.
-
Progressive superior migration leads to:
-
Superior glenoid erosion
-
Acromial wear
-
-
Conventional anatomic total shoulder arthroplasty fails in this setting due to early glenoid component loosening.
Clinical Features of Cuff Tear Arthropathy
-
Chronic shoulder pain associated with weakness.
-
Markedly reduced active range of motion with near-normal passive motion.
-
Crepitus during shoulder movement.
-
Pseudoparalysis, particularly of forward elevation.
-
Occasionally, large subdeltoid effusions.
-
Forward elevation is significantly limited.
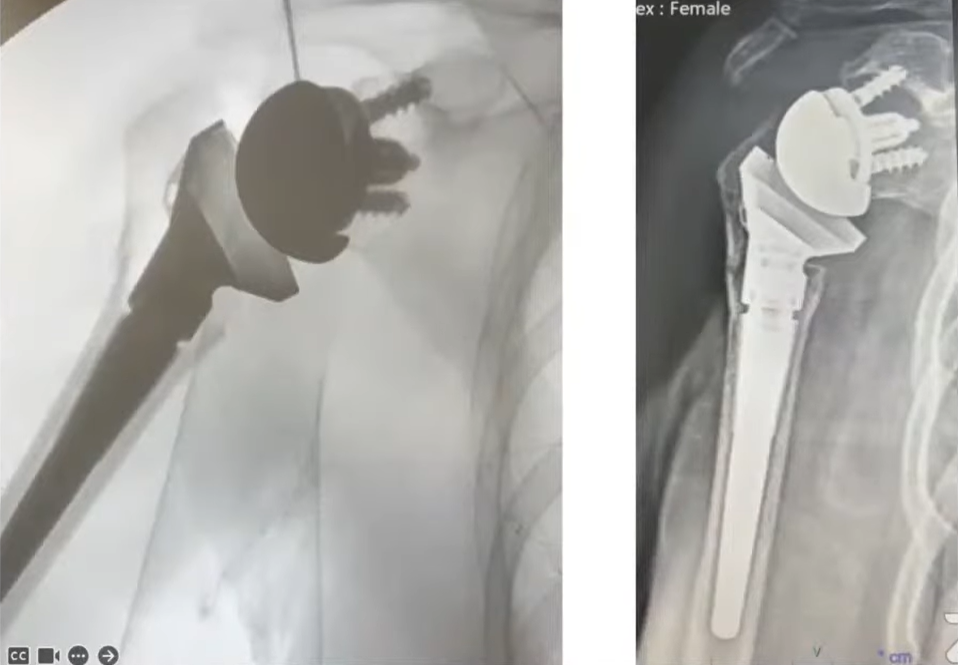
Radiographic Features
-
Superior migration of the humeral head.
-
Formation of an acromiohumeral pseudoarticulation.
-
Loss of normal glenohumeral joint space.
-
Erosion of the superior glenoid and the undersurface of the acromion.
-
Variable patterns of degenerative change.
Historical Treatment Approaches
-
Hemiarthroplasty was the standard treatment before the development of reverse total shoulder arthroplasty.
-
It provided reliable pain relief.
-
It failed to restore active forward elevation.
-
It did not correct the altered biomechanics of a cuff-deficient shoulder.
Indications for Reverse Total Shoulder Arthroplasty
-
Nonfunctional or irreparable rotator cuff.
-
Cuff tear arthropathy.
-
Pseudoparalysis due to massive rotator cuff tear without established arthritis.
-
Multiple failed rotator cuff repairs with associated instability.
-
Three- or four-part proximal humeral fractures in elderly patients.
-
Proximal humeral nonunions and tuberosity malunions.
-
Failed shoulder arthroplasty associated with rotator cuff insufficiency.
Ideal Patient Selection
-
Intact and functioning deltoid muscle.
-
Adequate glenoid bone stock to permit secure baseplate fixation.
-
Absence of active infection.
-
No severe neurologic disorders such as Parkinson disease, Charcot joint, or syringomyelia.
-
Functional demands compatible with implant longevity.
Contraindications
-
Absent or nonfunctional deltoid muscle.
-
Severe glenoid bone loss precluding stable baseplate fixation.
-
Active infection.
-
Relative contraindication: limited surgeon experience with the procedure.
Age Considerations
-
Historically avoided in patients younger than seventy years.
-
Current practice accepts use in selected younger patients with end-stage pathology.
-
Outcomes are influenced more by indication than by age alone.
Biomechanics of Reverse Total Shoulder Arthroplasty
-
Reverses the normal ball-and-socket configuration of the shoulder.
-
Medializes and distalizes the center of rotation.
-
Converts the shoulder into a deltoid-powered joint.
-
Prevents superior migration of the humerus during deltoid contraction.
-
Creates a semiconstrained fulcrum to allow shoulder elevation.
Glenoid Fixation Considerations
-
High shear stresses are transmitted across the glenoid baseplate.
-
Accurate baseplate positioning is essential.
-
The inferior screw experiences the highest shear forces.
-
Optimal fixation is achieved by engaging dense cortical bone in:
-
The coracoid base
-
The inferior scapular pillar
-
The scapular spine
-
Lateralized Center of Rotation
-
Increases the bending moment at the glenoid–implant interface.
-
Still allows secure fixation when properly implanted.
-
Reduces the incidence of scapular notching.
Glenoid Wear Patterns
-
Glenoid wear is common in cuff-deficient shoulders.
-
Recognized patterns include:
-
Posterior wear
-
Superior wear
-
Global wear
-
Anterior wear
-
-
These patterns influence surgical technique and screw trajectory.
Management of Glenoid Deficiency
-
Use of alternative center-line screw placement along the scapular spine.
-
Bone grafting when required.
-
Use of larger glenospheres.
-
Availability of augmented glenoid components.
-
Clinical outcomes are comparable to those achieved in patients with normal glenoid bone stock.
Overall Outcomes of Reverse Total Shoulder Arthroplasty
-
Clinical results vary depending on indication.
-
Posttraumatic and revision cases show inferior outcomes.
-
Absence or fatty infiltration of the teres minor muscle negatively affects results.
-
Good to excellent outcomes are reported in approximately sixty-seven to eighty-two percent of patients.
Functional Outcomes
-
Significant improvement in pain scores.
-
Average postoperative forward elevation ranges from one hundred to one hundred thirty-eight degrees.
-
Many patients return to medium- and high-demand daily activities.
Implant Survivorship
-
Approximately ninety percent at ten years.
-
Approximately eighty-seven percent at fifteen years.
-
Glenoid component survivorship is approximately eighty-four percent.
Reverse Total Shoulder Arthroplasty for Cuff Tear Arthropathy
-
Provides excellent pain relief in most patients.
-
Marked improvement in active forward elevation.
-
High incidence of scapular notching.
-
Scapular notching typically does not correlate with implant loosening.
Comparative Outcomes
-
Reverse total shoulder arthroplasty is superior to hemiarthroplasty for cuff tear arthropathy.
-
Primary reverse total shoulder arthroplasty performs better than revision procedures.
Rotator Cuff Dysfunction Without Arthritis
-
Represents an expanded indication.
-
Demonstrates good mid- to long-term functional improvement.
-
Associated with higher complication rates, approximately twenty percent.
-
Implant survivorship is approximately ninety percent at four years.
Proximal Humeral Fractures in the Elderly
-
Particularly useful for comminuted three- and four-part fractures.
-
Average postoperative forward elevation is approximately one hundred degrees.
-
High incidence of scapular notching.
-
Meta-analyses demonstrate superiority over hemiarthroplasty.
Rheumatoid Arthritis with Rotator Cuff Tear
-
Improves pain and shoulder function.
-
Scapular notching occurs in approximately one-quarter of patients.
-
Low rates of component loosening.
-
Increased risk of intraoperative and postoperative fractures.
Salvage and Revision Arthroplasty
-
Inferior outcomes compared with primary reverse total shoulder arthroplasty.
-
Useful following failed arthroplasty or infection.
-
Patient satisfaction remains high, approximately ninety percent.
-
Risk of loss of motion if preoperative forward elevation exceeds ninety degrees.
Complications
-
Scapular notching.
-
Instability.
-
Infection.
-
Periprosthetic fracture.
-
Glenoid component loosening.
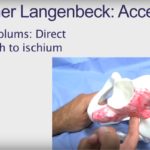
Surgical Approach
-
Proximal humeral exposure is similar to standard shoulder arthroplasty.
-
The deltopectoral approach is preferred due to versatility and extensile exposure.
-
A superior approach may be used but is less adaptable.
-
Adequate exposure of both the humerus and glenoid is mandatory.
Key Differences in Humeral Preparation
-
A larger humeral head cut is often required due to superior subluxation.
-
Proximal humeral migration is common in cuff-deficient shoulders.
-
Bone resection must restore appropriate deltoid tension without overlengthening.
Humeral Stem Version
-
Retroversion between twenty and thirty degrees is commonly used.
-
Thirty degrees of retroversion is preferred by many surgeons.
-
Increased retroversion reduces the risk of instability in adduction and extension.
Humeral Stem Fixation
-
Early designs used cemented stems.
-
Modern uncemented and short stems demonstrate favorable outcomes.
-
Stem choice depends on bone quality, fracture pattern, and surgeon preference.
Glenoid Preparation and Baseplate Placement
-
Complete debridement of the glenoid vault until all four borders are visible.
-
Identification of the true glenoid center.
-
Starting point shifted one to two millimeters inferiorly to reduce scapular notching.
-
Inferior edge of the baseplate should be flush with the inferior glenoid.
Guide Pin Placement and Reaming
-
Guide pin inserted with ten to fifteen degrees of inferior tilt.
-
Inferior tilt reduces scapular notching and improves longevity.
-
Reaming continues until the “smiley face” sign is achieved:
-
Bleeding cancellous bone inferiorly
-
Sclerotic bone superiorly
-
Glenosphere and Final Assembly
-
Morse taper must be thoroughly dried.
-
Glenosphere is securely impacted and stability confirmed.
-
Humeral components are trialed to assess stability, motion, and deltoid tension.
-
Slight increase in deltoid tension is acceptable.
-
Overlengthening must be avoided to prevent wound problems and acromial or scapular spine fractures.
Subscapularis Management
-
The role of subscapularis repair remains controversial.
-
Some studies show no clear relationship between repair and outcome.
-
Repair may improve stability in medialized designs.
-
Likely less critical in lateralized reverse total shoulder arthroplasty designs.
Key Surgical Pearls
-
Inferior baseplate placement and inferior tilt are essential to minimize scapular notching.
-
Avoid excessive deltoid lengthening.
-
Glenoid fixation quality is the primary determinant of long-term implant survival.
-
Thorough trialing is critical before final implantation.


Leave a Reply