Courtesy: Saqib Masud FRCS,John Davies FRCS
Overview
The anterior approach to the hip, commonly known as the Smith–Peterson approach, provides safe and direct access to the hip joint.
Indications
This approach is widely used for:
-
Hip joint procedures
-
Pelvic osteotomies
-
Total hip replacement (THR)
It also allows extension to the pelvis when required.
Patient Positioning
-
Patient is placed in the supine position
Modifications
For Pelvic Osteotomy
-
A small sandbag under the ipsilateral buttock improves exposure
For Total Hip Replacement
-
A traction table may be used to:
-
Facilitate limb positioning
-
Improve surgical access
-
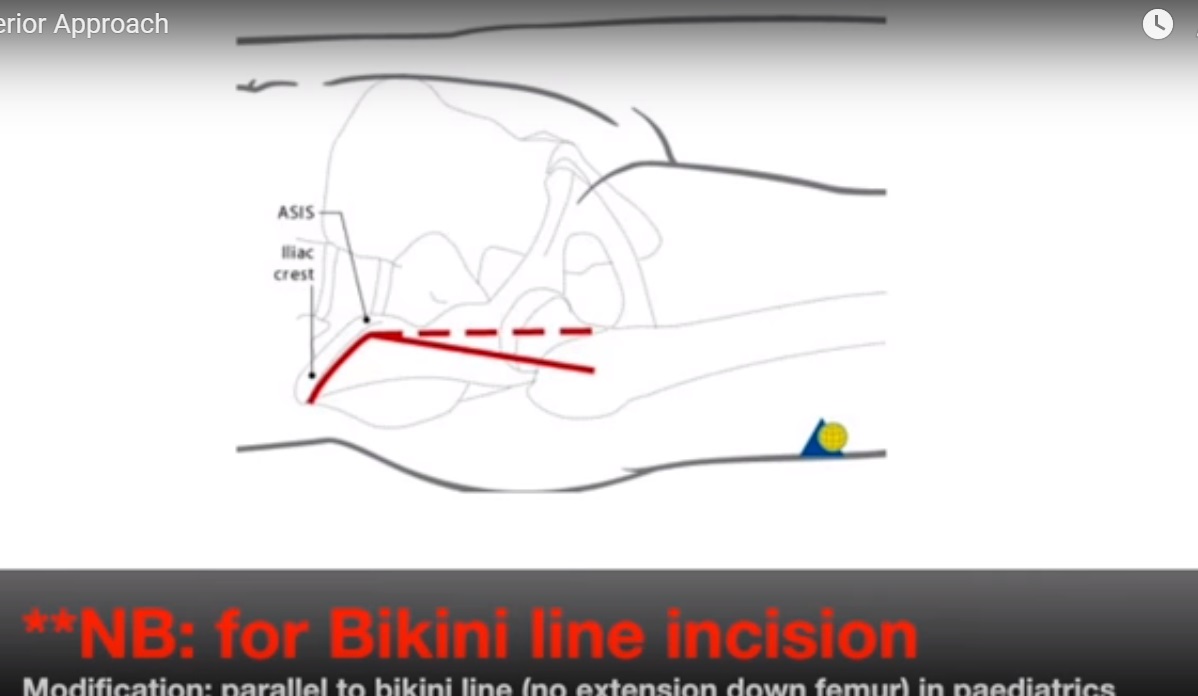
Surface Landmarks
Key anatomical landmarks guiding the incision:
-
Iliac crest
-
Anterior superior iliac spine (ASIS)
-
Shaft of the femur
These landmarks help determine the orientation of incision and dissection
Skin Incision
-
Begins over the anterior iliac crest
-
Extends toward the ASIS
-
Then curves distally for 8–10 cm along the anterior thigh
Internervous Plane
This approach utilizes a safe internervous interval:
| Muscle | Nerve Supply |
|---|---|
| Tensor fasciae latae | Superior gluteal nerve |
| Sartorius | Femoral nerve |
This allows muscle separation without denervation
Identification of the Intermuscular Interval
-
Interval lies between tensor fasciae latae (TFL) and sartorius
-
Best identified 5–7 cm distal to ASIS
Surgical Tip
-
External rotation of the leg makes the sartorius more prominent, aiding identification
Structures at Risk
Lateral Femoral Cutaneous Nerve (LFCN)
Location
-
Pierces deep fascia 2–3 cm medial and inferior to ASIS
Risk
-
Vulnerable during superficial dissection
Protection Strategies
-
Incise fascia medial to TFL
-
Stay within the TFL fascial sheath
Vascular Structures
-
Ascending branch of the lateral femoral circumflex artery lies within the interval
Must be identified and controlled to prevent bleeding
Muscle Retraction
After identifying the interval:
-
Tensor fasciae latae — retracted laterally
-
Sartorius (+ LFCN) — retracted medially
This exposes the deeper anterior hip structures
Deep Dissection
Intermuscular Plane
-
Between:
-
Gluteus medius (lateral)
-
Rectus femoris (medial)
-
Rectus Femoris Release
To improve exposure, rectus femoris is detached.
Origins
-
Direct head — Anterior inferior iliac spine (AIIS)
-
Reflected head — Superior acetabular rim
Neurovascular Structures at Risk
-
Femoral nerve
-
Femoral artery
Location
-
Medial to rectus femoris within the femoral triangle
Careful retraction is essential to avoid injury
Exposure of the Hip Joint
-
Iliopsoas muscle is retracted medially
-
This exposes the anterior hip capsule
Limb Positioning
-
Abduction
-
Full external rotation
Helps tension the capsule and facilitates exposure
Capsulotomy and Hip Dislocation
-
The anterior capsule is incised
-
Hip joint is then dislocated for surgical intervention
Extension of the Approach
Local Extension
Exposure can be increased by releasing:
-
Tensor fasciae latae
-
Sartorius
-
Gluteus medius
-
Gluteus minimus
Proximal Extension
-
Incision extended along the iliac crest
-
Allows access to:
-
Inner pelvis
-
Outer pelvis
-
Distal Extension
-
Extended along the anterolateral thigh
-
Provides access to the entire femoral shaft
Summary
-
The Smith–Peterson approach utilizes a safe internervous plane
-
Provides excellent exposure of:
-
Hip joint
-
Anterior pelvic structures
-
-
Key to success:
-
Accurate identification of landmarks
-
Protection of LFCN and femoral neurovascular structures
-
-
Approach is highly versatile, allowing proximal and distal extension as needed
.

Leave a Reply