Courtesy: Prof Nabil Ebraheim, University of Toledo, Ohio, USA
-
ACL Tear: Clinical and Radiological Diagnosis
Introduction
Anterior cruciate ligament (ACL) injury is one of the most common ligament injuries of the knee, particularly in athletes involved in pivoting sports.
Early and accurate diagnosis is essential to:
- Restore knee stability
- Prevent secondary meniscal injury
- Reduce long-term osteoarthritis risk
- Guide appropriate treatment planning
Diagnosis is based on a combination of:
- Clinical examination
- Radiographic evaluation
- MRI findings
Anatomy and Function of the ACL
The ACL is a:
- Central intra-articular ligament of the knee
Its primary functions are to prevent:
- Anterior translation of the tibia
- Rotational instability
The ACL is also an important stabilizer during:
- Pivoting movements
- Deceleration activities
- Cutting maneuvers
Mechanism of Injury
Most ACL injuries occur through:
- Non-contact pivoting mechanisms
Common injury scenarios include:
- Sudden deceleration
- Twisting with the foot planted
- Landing awkwardly after jumping
- Rapid change in direction
These mechanisms commonly produce:
- Rotational valgus stress on the knee
Clinical Presentation
Typical symptoms of ACL injury include:
- Audible or felt “pop”
- Immediate deep knee pain
- Rapid swelling due to hemarthrosis
- Instability or giving-way sensation
Hemarthrosis
Rapid swelling occurs because of bleeding from:
- Middle genicular artery injury
Hemarthrosis developing within a few hours strongly suggests:
- Intra-articular ligament injury
Clinical Examination
Gait Pattern
Patients may demonstrate:
- Quadriceps avoidance gait
This occurs because the patient attempts to minimize anterior tibial translation during walking.
Lachman Test
Most Sensitive Clinical Test
The Lachman test is considered the:
- Most sensitive examination test for ACL injury
Technique
- Knee flexed to approximately 20–30°
- Examiner stabilizes femur
- Tibia is pulled anteriorly
Positive Findings
- Increased anterior tibial translation
- Soft or absent endpoint
Radiological Evaluation
Role of X-Rays
Plain radiographs may identify:
- Associated fractures
- Avulsion injuries
- Indirect signs of ACL rupture
Although X-rays do not directly visualize the ACL, they are important in the initial evaluation.
X-Ray Findings Associated with ACL Injury
ACL Avulsion Fracture
The ACL may avulse from the:
- Tibial eminence (tibial spine)
This is more commonly seen in:
- Children and adolescents
The injury may be visualized on:
- AP view
- Lateral view
Tibial Spine Fracture
Tibial spine fractures are considered the:
- Pediatric equivalent of ACL rupture
because the immature bone fails before the ligament itself.
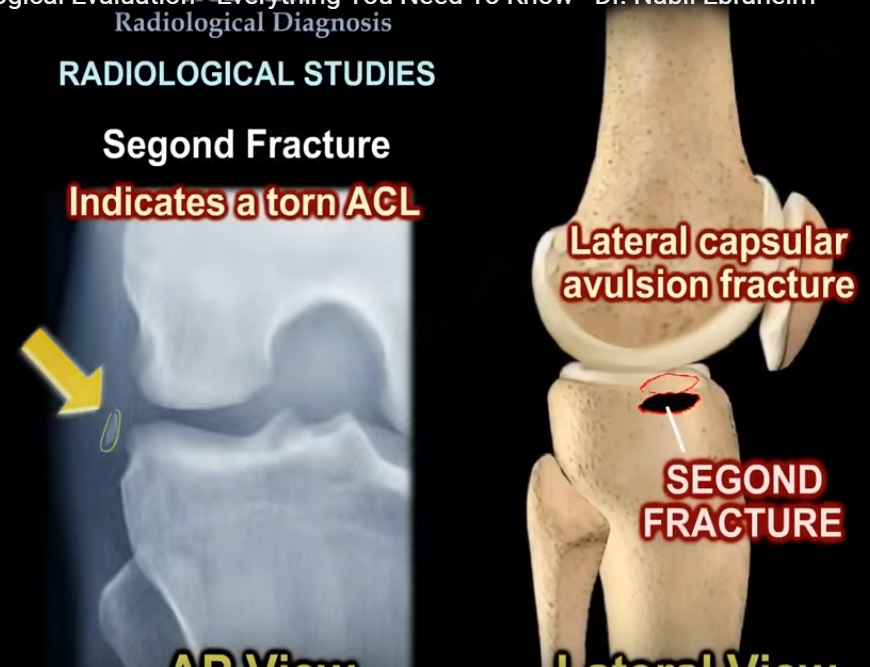
Segond Fracture
Definition
A Segond fracture is:
- A small avulsion fracture from the lateral tibial plateau
Clinical Significance
It is strongly associated with:
- ACL tears
and should always prompt evaluation for associated ligament injury.
Lateral Femoral Notch Sign
This refers to:
- An impaction fracture or depression of the lateral femoral condyle
Diagnostic Criteria
A sulcus depth greater than:
- 2 mm
is considered suggestive of ACL injury.
Arcuate Fracture
Definition
An arcuate fracture is:
- An avulsion fracture of the fibular head
Clinical Importance
It indicates possible injury to the:
- Posterolateral corner (PLC)
and is commonly associated with:
- ACL injuries
- PCL injuries
Important Clinical Pearl
Failure to recognize associated posterolateral corner injury may lead to:
- Failure of ligament reconstruction
MRI Evaluation
Gold Standard Imaging
MRI is considered the:
- Gold standard investigation for ACL tears
It provides excellent visualization of:
- Ligament integrity
- Bone bruising
- Meniscal injury
- Associated soft tissue pathology
Direct MRI Signs of ACL Tear
Fiber Disruption
The ACL fibers appear:
- Discontinuous
- Torn
- Irregular
Non-Visualization of the ACL
In complete tears:
- ACL fibers may not be visualized
Wavy or Dangling Fibers
Partial or proximal tears may show:
- Retracted proximal fibers
- Sagging distal fibers
Empty Notch Sign
Definition
Absence of ACL tissue within the:
- Intercondylar notch
Significance
Typically indicates:
- Proximal femoral avulsion of the ACL
Indirect MRI Signs of ACL Tear
Bone Bruise Pattern
One of the most important indirect MRI findings is the classic:
- Lateral compartment bone bruise pattern
Typical Locations
Bone bruising commonly involves:
- Mid lateral femoral condyle
- Posterior lateral tibial plateau
This pattern is highly suggestive of:
- Pivot-shift injury mechanism
Anterior Tibial Translation
MRI may demonstrate:
- Anterior displacement of the tibia relative to the femur
PCL Buckling
Secondary changes may include:
- Buckling or increased curvature of the posterior cruciate ligament (PCL)
This occurs due to altered knee mechanics after ACL rupture.
Associated Injuries
Acute ACL Tears
Acute ACL injuries are more commonly associated with:
- Lateral meniscus tears
Chronic ACL Deficiency
Chronic ACL instability more commonly leads to:
- Medial meniscus tears
Biomechanical Explanation
The posterior horn of the medial meniscus functions as a:
- Secondary stabilizer of the knee
In chronic ACL deficiency:
- Increased stress is transferred to the medial meniscus
- This predisposes it to tearing
Importance of Combined Clinical and Radiological Assessment
MRI findings must always be correlated with:
- Clinical examination
- Mechanism of injury
- Patient symptoms
Not all MRI abnormalities are clinically significant.
Similarly:
- Clinical instability may exist despite subtle imaging findings
Key Clinical Pearls
- Lachman test is the most sensitive clinical test for ACL injury.
- Segond fracture is strongly associated with ACL rupture.
- Tibial spine fracture is the pediatric equivalent of ACL tear.
- Classic MRI bone bruise pattern involves the lateral compartment.
- Acute ACL tears commonly involve the lateral meniscus.
- Chronic ACL deficiency commonly leads to medial meniscus injury.
- Posterolateral corner injuries must not be missed.
Final Take-Home Message
ACL injury diagnosis requires a careful combination of:
- Clinical examination
- Plain radiography
- MRI assessment
Understanding both direct and indirect radiological signs is essential for:
- Accurate diagnosis
- Detection of associated injuries
- Surgical planning
Early recognition and treatment help restore knee stability, reduce secondary joint damage, and improve long-term outcomes.
Thank you very much for informative n practical points.Is fibular head n fibular styloid process both r same r different?Arcuate sign .