Courtesy: Prof Nabil Ebraheim, University of Toledo, Ohio, USA
Radial Head and Neck Fractures in Children
Overview
- Uncommon pediatric elbow injury.
- Peak incidence around 9 years of age.
- Usually caused by a valgus force following a fall on an outstretched hand.
Types of Fractures
- Non displaced fractures.
- Displaced fractures.
- Angulated (tilted) fractures.
- Translocated fractures.
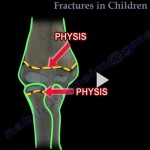
Location
- Physeal fractures (Salter Harris injuries).
- Metaphyseal fractures (radial neck fractures).
Ossification Centers Around the Elbow (CRITOE)
Mnemonic: CRITOE (1, 3, 5, 7, 9, 11 years)
- Capitellum – 1 year.
- Radial head – 3 years.
- Internal (medial) epicondyle – 5 years.
- Trochlea – 7 years.
- Olecranon – 9 years.
- External (lateral) epicondyle – 11 years.
Imaging
Standard views
- Anteroposterior and lateral radiographs of the elbow.
- Include the forearm in the radiographs.
Radiological rule
- The radial head must align with the capitellum on every radiographic view.
Radiocapitellar view
- Elbow flexed to 90 degrees.
- Thumb pointing upward.
- X ray beam angled 45 degrees proximally.
Fat pad sign
- Posterior fat pad is always abnormal and indicates an occult fracture.
- May be absent in extra articular radial neck fractures.
Acceptable Angulation
- Angulation of 30 degrees or less is generally acceptable.
Treatment
Non displaced fractures or angulation 30 degrees or less
- Immobilization alone.
Fractures with angulation greater than 30 degrees
- Closed reduction.
Closed reduction technique
- Longitudinal traction.
- Forearm supination.
- Elbow extension.
- Varus stress.
- Direct pressure on the radial head medially and the shaft laterally.
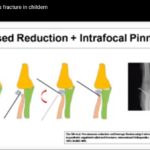
If closed reduction fails
- Percutaneous reduction using a K wire joystick technique.
Open reduction
- Reserved as the final option.
- Consider only when residual angulation exceeds 45 degrees after closed and percutaneous reduction.
- Avoid whenever possible because of the higher complication rate.
Fixation
- K wire fixation may be used following reduction when required.
Complications
- Radioulnar synostosis, particularly after excessive dissection or open reduction.
- Loss of forearm rotation, especially pronation and supination.
- Osteonecrosis of the radial head due to vascular injury.
- Nonunion, usually caused by periosteal interposition.
Important Clinical Points
- Complication rates increase after open reduction.
- Outcomes are generally poorer in children older than 10 years.
Clinical Pearls
- Always confirm radiocapitellar alignment.
- A posterior fat pad sign should be considered evidence of an occult fracture until proven otherwise.
- Follow the treatment sequence of closed reduction, then percutaneous reduction, and finally open reduction if necessary.
- Perform repeated neurovascular examinations.
- Monitor for compartment syndrome, particularly if increasing analgesic requirements are noted.
Exam Pearls
- CRITOE ossification sequence: 1, 3, 5, 7, 9, 11 years.
- Angulation of 30 degrees or less is treated with immobilization.
- Angulation greater than 30 degrees requires reduction.
- Residual angulation greater than 45 degrees after reduction may require open reduction.
- The radial head should always align with the capitellum on every radiographic view.
- Posterior fat pad sign indicates an occult fracture.
- Open reduction should be the last treatment option because of its higher complication rate.

Leave a Reply