Courtesy: Prof Nabil Ebraheim, University of Toledo, Ohio, USA
GENERAL OVERVIEW
-
Radial head and radial neck fractures in children are uncommon injuries.
-
These fractures typically occur around 9 years of age.
-
The usual mechanism of injury is a valgus force applied to the elbow.
-
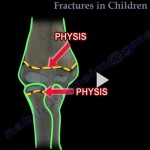
Fractures may involve:
-
The physis (growth plate) of the radial head
-
The metaphysis of the radial neck
-
TYPES OF FRACTURES
Radial head and neck fractures may be:
-
Non-displaced
-
Displaced
-
Tilted
-
Translocated
OSSIFICATION CENTERS OF THE ELBOW (CRITOE)
Knowledge of ossification centers is essential to avoid misdiagnosis.
-
1 year: Capitellum
-
3 years: Radial head
-
5 years: Internal (medial) epicondyle
-
7 years: Trochlea
-
9 years: Olecranon
-
11 years: External (lateral) epicondyle
RADIOLOGICAL EVALUATION
Plain Radiographs
-
Anteroposterior view
-
Lateral view
Radiocapitellar (Greenspan) View
-
An oblique lateral view
-
Elbow flexed to 90 degrees
-
Thumb pointing upward
-
X-ray beam directed at 45 degrees
-
Useful for visualizing subtle radial head and neck injuries
Computed Tomography
-
Used selectively
-
Helpful in complex or unclear fractures
IMPORTANT RADIOLOGICAL SIGNS
Fat Pad Sign
-
Non-displaced radial head fractures may not be visible on initial radiographs.
-
Presence of a posterior fat pad is abnormal and indicates an occult fracture.
Radial Neck Fractures
-
Partially extra-articular.
-
Fat pad sign may be absent, even in the presence of a fracture.
TREATMENT PRINCIPLES
Non-Displaced Fractures
-
Managed with immobilization.
-
Immobilization is acceptable when angulation is less than 30 degrees.
-
Angulation up to 30 degrees is generally well tolerated in children.
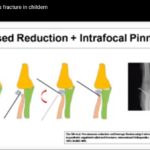
Displaced Fractures
Closed Reduction
-
Indicated when angulation is greater than 30 degrees.
-
Reduction techniques include:
-
Elastic bandage wrapped around the forearm and elbow
-
Elbow extension with traction
-
Supination and varus force
-
Direct pressure over the radial head to push it medially
-
Lateral displacement of the radial shaft
-
-
After reduction, the radial head often remains stable due to the intact periosteum.
Percutaneous Reduction
-
A Kirschner wire may be used as a joystick for manipulation.
-
Useful when closed manipulation alone is insufficient.
Open Reduction
-
Reserved for cases where:
-
Closed and percutaneous reduction fail
-
Residual angulation remains greater than 45 degrees
-
-
Should be avoided when possible due to higher complication rates.
COMPLICATIONS
-
Radioulnar synostosis
-
Loss of elbow motion, particularly forearm rotation
-
Osteonecrosis of the radial head
-
Non-union or malunion
KEY POINTS
-
Most pediatric radial neck fractures can be managed non-operatively.
-
Accurate assessment of angulation is critical.
-
Gentle reduction techniques reduce the risk of complications.
-
Open reduction should be the last resort.
-
Early mobilization after healing helps restore motion.

Leave a Reply