Courtesy:
Rakesh Mashru, MD. Cooper Medical School at Rowan University, Department of Orthopaedic Surgery.
General Principles of Pediatric Trauma (Orthopaedic Focus)
1. Epidemiology
Fracture Incidence
- By age 16:
- ~40% of males
- ~25% of females
– sustain at least one fracture
Most Common Fracture Sites
- Distal forearm (wrist)
- Clavicle
2. How Children Differ from Adults
A. Bone Properties
- Pediatric bone is:
- More elastic
- Less brittle
Clinical Implication
- Leads to:
- Plastic deformation (bending without fracture)
- Incomplete fractures
Types of Pediatric Fractures
- Greenstick fracture
- Buckle (torus) fracture
- Plastic deformation
B. Stress–Strain Behavior
- Adults:
- Sudden failure after yield point
- Children:
- Bone bends before breaking
Result
- Unique fracture patterns
- Incomplete fractures
3. Remodeling and Overgrowth Potential
Remodeling Ability
- Very high in children
- Deformities may correct over time
Factors Affecting Remodeling
- Age:
- Younger – better remodeling
- Plane of deformity:
- Sagittal > Coronal
- Distance from physis:
- Closer – better remodeling
- Growth potential:
- Knee > Hip
Overgrowth Phenomenon
- Common in:
- Femoral shaft fractures
Effect
- Can correct up to ~2 cm shortening
Mechanism
- Increased blood flow (hyperemia) – stimulates growth
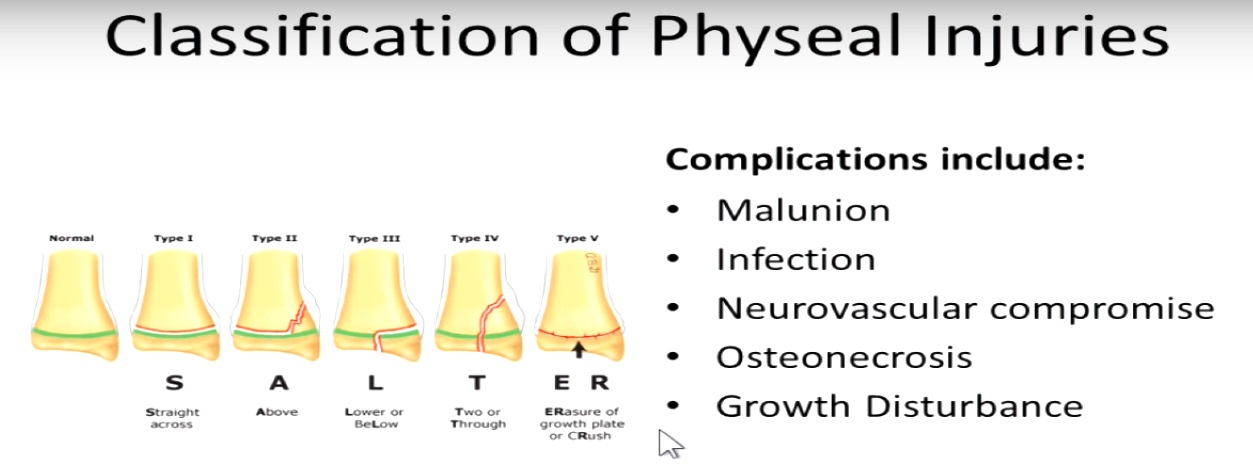
4. Physeal (Growth Plate) Injuries
Incidence
- ~20% of pediatric fractures
Common Age Group
- 8–14 years
Risk of Growth Arrest
- ~1–10%
Salter-Harris Classification (High-Yield)
- Type I – Through physis
- Type II – Above physis
- Type III – Below physis
- Type IV – Through all layers
- Type V – Crush injury
5. Pediatric Polytrauma Principles
Initial Assessment
- Follow ABC approach:
- Airway
- Breathing
- Circulation
Important Concept
- Children are not small adults
Key Differences
- Delayed signs of shock
- Instability appears after 20–30% blood loss
- Better initial compensation
- Sudden deterioration possible
6. Trauma Scoring Systems
A. Injury Severity Score (ISS)
- Based on 6 body regions
- Score >16 – Polytrauma
B. Pediatric Trauma Score (PTS)
Parameters
- Weight
- Airway
- Blood pressure
- CNS status
- Fractures
- Skin injury
Interpretation
-
8 – Low mortality
C. Pediatric Glasgow Coma Scale (GCS)
- Modified for:
- Verbal response
- Age differences
7. Child Abuse (Non-Accidental Injury)
Incidence
- ~1–2% of children annually
Red Flags
- Fracture in non-ambulatory child
- Multiple fractures at different stages
- Inconsistent history
Suspicious Fractures
- Femoral shaft fractures (infants)
- Hand and foot fractures
- Metaphyseal corner fractures
- Posterior rib fractures
8. Special Pediatric Injury Patterns
A. SCIWORA
(Spinal Cord Injury Without Radiographic Abnormality)
- Seen in children
- Due to:
- Ligamentous laxity
- Elastic spine
Key Feature
- X-ray: Normal
- MRI: Abnormal
B. Pediatric Pelvic Fractures (Torode & Zieg Classification)
- Type I – Avulsion injuries
- Type II – Iliac wing fractures
- Type III – Stable pelvic ring
- Type IV – Unstable pelvic ring
9. Management Principles
General Approach
- Follow Damage Control Orthopaedics
Priority Order
- Life
- Limb
- Function
Key Steps
- Resuscitation (ABC first)
- Neurovascular assessment
- Open fracture care:
- Debridement
- Stabilization
Gold Standard in Pediatrics
- Closed reduction + casting
Exam Tip
- If unsure – choose closed reduction
10. Final Take-Home Points
- Children have:
- Better healing
- Better remodeling
Acceptable Deformity
- Mild angulation
- Mild shortening
Always Remember
- Rule out physeal injury
- Consider child abuse
Core Principle
- Trauma care:
- Same principles as adults
- But different physiology
Final Message
- Successful pediatric trauma management depends on:
- Understanding growth biology
- Recognizing unique injury patterns
- Applying age-appropriate treatment strategies
Leave a Reply