Courtesy: Saqib Rehman MD, Associate Professor, Director of Orthopaedic Trauma, Temple University, Philadephia, Pennsylvania, USA
Pediatric Trauma Panel Discussion
Posterior Hip Dislocation in Adolescents
Key points
- Commonly caused by high energy trauma such as sports injuries and road traffic accidents.
- Usually occurs in adolescents with open physes.
- Always assess for associated femoral head injury.
- Always assess for acetabular fracture.
- Always assess for physeal injury (Salter Harris Type I).
Important concept
- Forceful reduction may cause physeal separation of the femoral head.
- This represents an iatrogenic Salter Harris Type I injury.
Management
- Posterior hip dislocation is an orthopaedic emergency.
- Reduce the hip ideally within 6 hours to reduce the risk of avascular necrosis.
- Gentle reduction is preferred.
- Reduction in the operating room may provide better control.
- Fluoroscopy may be useful during reduction.
Post reduction imaging
- Pelvic radiographs.
- CT scan to identify associated fractures.
- MRI in children to detect labral injuries and osteochondral lesions.
Complication
- Avascular necrosis is the most important complication.
- Risk increases with delayed reduction.
- Risk increases with associated physeal injury.
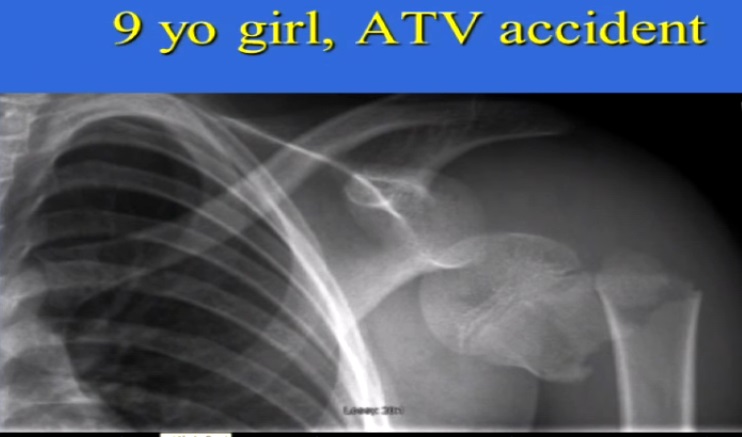
Proximal Humerus Fracture with Shoulder Dislocation
Case summary
- Rare injury combination in children.
- More commonly seen in a 9 year old child.
Important concept
- Shoulder dislocations are uncommon in children.
- Physeal or metaphyseal fractures are more common than pure dislocations.
Management
- Urgent closed reduction of the shoulder should be performed first.
- Fracture treatment is guided by the excellent remodeling potential of the proximal humerus.
Acceptable alignment (approximately 9 years of age)
- Up to 100 percent displacement may be accepted.
- Up to 40 to 50 degrees of angulation may be acceptable.
- Varus deformity greater than 35 to 40 degrees should be avoided.
Indications for surgery
- Irreducible shoulder dislocation.
- Severe malalignment.
- Older children, particularly over 12 years of age.
Fixation
- Percutaneous pinning when surgical fixation is required.
- Technically demanding procedure.
Outcome
- Excellent remodeling potential.
- Good functional recovery despite imperfect reduction.
Remodeling Potential of the Proximal Humerus
Key concept
- Approximately 80 percent of humeral growth occurs at the proximal humeral physis.
- This provides exceptional remodeling capacity in children.
Adolescent Femoral Shaft Fractures
Retrograde femoral nailing
- Contraindicated when the distal femoral physis remains open.
- Avoid if more than 2 years of growth remain.
- Appropriate only in skeletally mature adolescents.
Complication
- Growth arrest.
- Limb length discrepancy.
Exam Pearls
- Posterior hip dislocation requires emergency reduction within 6 hours.
- Physeal injury during reduction is an important pediatric concern.
- MRI is superior to CT for detecting labral and cartilage injuries.
- Proximal humerus fractures in children usually require nonoperative treatment.
- Children younger than 10 years have remarkable remodeling potential.
- Accept substantial displacement and angulation in younger children.
- Avoid retrograde femoral nailing in patients with an open distal femoral physis.

Leave a Reply