Courtesy: Dr Kowshik Jain, FRCS Tr and Orth, Dudley, UK
Ankle Arthroscopy: Indications, Technique, and Clinical Pearls
Introduction
- Speaker: Dr. Koshik Jane
- Affiliation:
- Dudley Group NHS Foundation Trust
- Midland Orthopaedic Centre
- Expertise:
- Foot and ankle surgery
- Arthroscopy
- Trauma and reconstruction
Overview
Ankle arthroscopy is a minimally invasive surgical procedure increasingly considered a core skill for foot and ankle surgeons.
Types
- Anterior ankle arthroscopy
- Posterior ankle arthroscopy (separate entity)
Historical Background
- Arthroscopy pioneered by Masaki Watanabe
- First ankle arthroscopy: Kenji Takagi (1939)
- Major advancement: Watanabe series (1972)
Indications for Ankle Arthroscopy
1. Impingement Syndromes
- Anterior or posterior
- Soft tissue or bony (osteophytes)
- “Kissing lesions” (tibia and talus)
2. Osteochondral Lesions
- Commonly talar lesions
- Gold standard treatment: arthroscopic microfracture
3. Septic Arthritis
- Arthroscopic washout preferred
4. Ankle Instability
- Detect associated intra-articular pathology:
- Osteochondral lesions
- Loose bodies
- Often combined with ligament repair
5. Loose Bodies
- Easily removed arthroscopically
6. Syndesmotic Injury
- Arthroscopy is the gold standard for diagnosis
- Useful when imaging is inconclusive
7. Arthritis
- Debridement
- Osteophyte removal
- Arthroscopic ankle fusion (excellent outcomes)
8. Fracture Assessment
- Limited role in assessing reduction
Contraindications
Absolute
- Local soft tissue infection
Relative
- Severe joint contracture
Equipment
Arthroscope Options
- 2.7 mm scope:
- Preferred (less cartilage damage)
- 4 mm scope:
- Better visualization
- Higher risk of cartilage injury
Tourniquet
- Thigh tourniquet commonly used
Fluid System
- Gravity inflow (preferred)
- Pump system:
- Advantage: improved hemostasis
- Risk: fluid extravasation, compartment syndrome
Anesthesia
- General anesthesia (most common)
- Regional anesthesia (alternative)
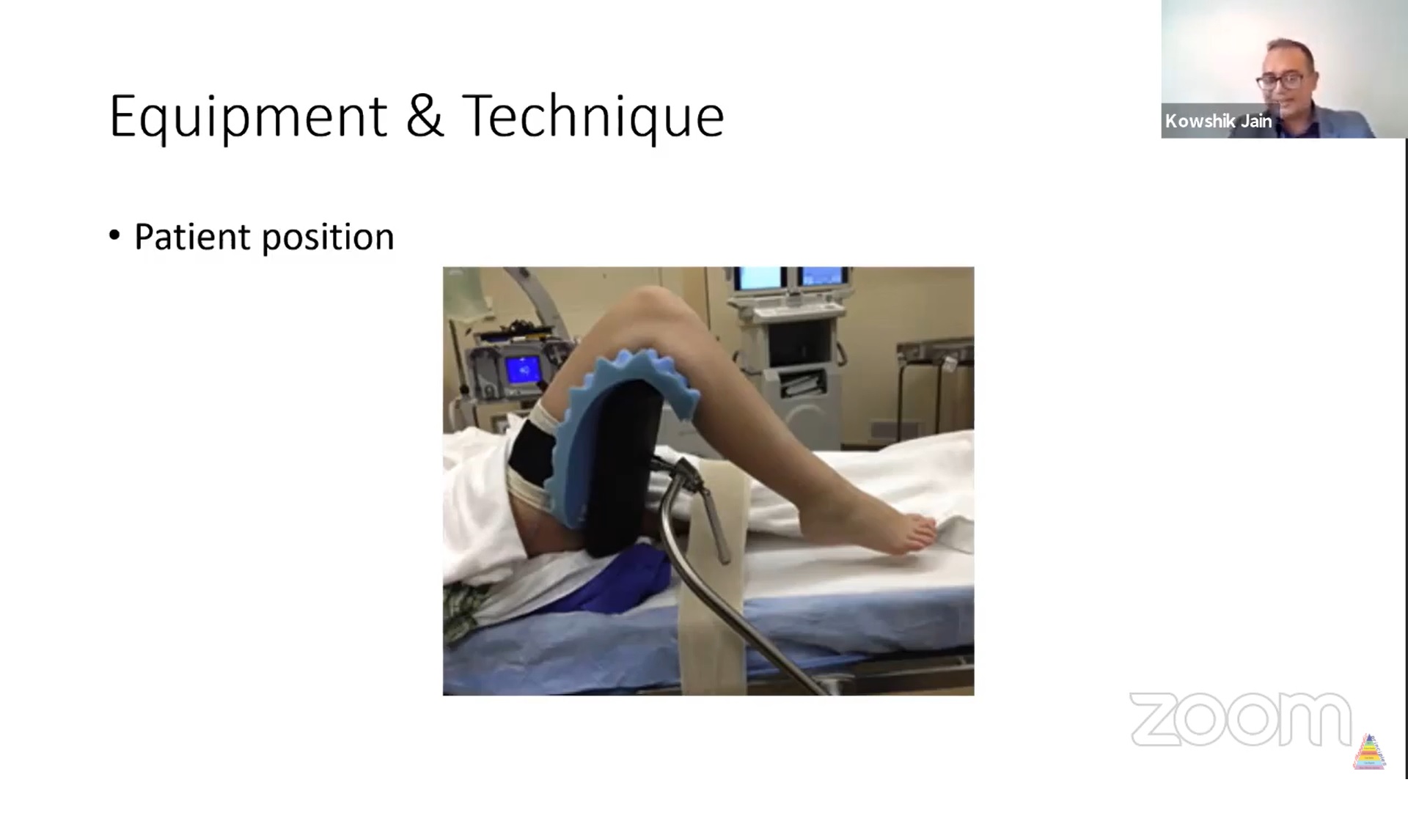
Patient Positioning
- Supine position
- Use of thigh holder (thigh gutter)
Key Points
- Adequate padding
- Prevent external rotation (use sandbag support)
Ankle Distraction
Types
- Non-invasive (preferred)
- Invasive (calcaneal pin – rarely used now)
Role
- Not always mandatory
- Improves:
- Joint space
- Visualization
Portal Anatomy (Critical for Safety)
Anteromedial Portal
- Medial to tibialis anterior tendon
Structures at Risk
- Saphenous nerve and vein
Anterolateral Portal
- Lateral to peroneus tertius or extensor digitorum longus tendon
Structures at Risk
- Superficial peroneal nerve (most commonly injured)
Posterolateral Portal
- Lateral to Achilles tendon
Structures at Risk
- Sural nerve
Surgical Technique
Step 1: Joint Entry
- Inject approximately 20 ml saline
- Confirms intra-articular placement
Step 2: Portal Creation
- Use “nick and spread” technique
- Minimizes injury to:
- Nerves
- Vessels
- Tendons
Step 3: Scope Introduction
- Typically through anteromedial portal
Step 4: Systematic Examination
- Use 21-point inspection system
- Evaluate:
- Anterior compartment
- Central compartment
- Posterior compartment
Step 5: Portal Switching
- Essential for optimal visualization
- Improves viewing angles:
- Anteromedial ? mediolateral view
- Anterolateral ? anteroposterior view
Important Surgical Tips
- Prevent limb external rotation
- Ensure adequate padding of thigh holder
- Mark superficial peroneal nerve before incision
- Mark portals prior to distraction
- Use “nick and spread” technique
- Always switch portals
- Remove distraction when working in anterior gutter
Complications
Overall Rate
- Approximately 2–5%
Common Complications
- Nerve injury (most common):
- Superficial peroneal nerve
- Infection (<1%)
- Tendon injury (extensor digitorum longus)
- Tourniquet-related pain
- Postoperative swelling (common, self-limiting)
- Joint stiffness (rare)
- Complex Regional Pain Syndrome (rare but serious)
Key Clinical Pearls
- Technically demanding procedure
- Thorough anatomical knowledge is essential
- Always perform systematic joint inspection
- Distraction is helpful but not mandatory
Recommended Early Cases for Beginners
- Soft tissue impingement
- Loose body removal
Advanced Applications
- Arthroscopic ligament repair
- Arthroscopic ankle fusion (>90% success rate)
- Syndesmotic assessment and reduction
Take-Home Message
- Ankle arthroscopy is:
- Safe
- Effective
- Increasingly essential
Success Depends On
- Proper technique
- Precise anatomical knowledge
- Systematic surgical approach



Leave a Reply