Courtesy: Dr Rajiv Limaye, FRCS Tr and Orth, Consultant Orthopaedic Surgeon, UK
Overview
Chronic ligament injuries of the ankle are a common orthopaedic problem encountered in:
- Emergency settings
- Routine clinical practice
- Sports medicine
Clinical Importance
These injuries can lead to:
- Persistent pain
- Instability
- Loss of sports and recreational activity
Anatomy Review
Bones Involved
- Tibia
- Fibula
- Talus
- Calcaneus (supporting structure)
Ligaments
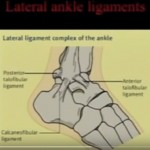
Lateral Ligament Complex (Most Commonly Injured)
- Anterior talofibular ligament (ATFL)
- Calcaneofibular ligament (CFL)
- Posterior talofibular ligament (PTFL)
Medial Ligament
- Deltoid ligament
- Superficial component
- Deep component
Stabilizers of the Ankle
Static Stabilizers
- Bony architecture
- Ligaments:
- ATFL — prevents anterior translation and inversion
- CFL — resists varus tilt
- PTFL — posterior stability
Dynamic Stabilizers
- Surrounding muscles (especially peroneals)
Biomechanics of Injury
| Mechanism | Resulting Injury |
|---|---|
| Inversion + internal rotation | ATFL – PTFL injury |
| Varus stress + rotation | CFL injury |
| External rotation | Deltoid ligament injury |
| Dorsiflexion force | PTFL / posterior injury |
| External rotation + syndesmotic stress | High ankle sprain |
Epidemiology
- 10–40% of athletic injuries involve the ankle
- 80% are lateral ligament injuries
- 20% are medial injuries
- 10–30% progress to chronic instability
Pathogenesis
- 70–80% of acute injuries heal adequately
- Failure of healing leads to:
- Ligament elongation
- Recurrent sprains
- Chronic instability
Instability vs Laxity
Functional Instability (Subjective)
- Sensation of “giving way”
- Lack of confidence in the ankle
- No objective laxity
Mechanical Instability (Objective)
- Demonstrable on clinical testing
- True ligament laxity
Clinical Evaluation
History
- Mechanism of injury
- Previous ankle injuries
- Pain and swelling
- Ability to bear weight
Examination
Inspection
- Swelling
- Bruising
- Deformity
Palpation
- Ligament tenderness
- Bone tenderness
- Tendons and neurovascular status
Range of Motion
- Plantarflexion
- Dorsiflexion
- Inversion / eversion
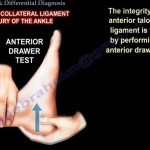
Special Tests
Anterior Drawer Test
- Assesses ATFL
- Positive finding:
- Increased anterior translation
- “Suction sign”
Talar Tilt Test
- Assesses CFL
Syndesmotic Tests
- Squeeze test
- External rotation test
Generalized Laxity
- Beighton score >/= 7 suggests hyperlaxity
Imaging
X-ray
- Weight-bearing views preferred
MRI
- Detects:
- Osteochondral lesions
- Deltoid ligament injury
- Bone edema
Ultrasound
- Useful for:
- Tendons
- Soft tissue
Stress Views
- Helpful in chronic instability
Management
Acute Phase (Conservative Management)
Principles
- Rest
- Ice
- Compression
- Elevation
Support
- Walking boot or brace (4–6 weeks)
Weight Bearing
- As tolerated
Physiotherapy
- Peroneal strengthening
- Proprioception training
- Gastrosoleus stretching
Rehabilitation
Early Phase
- Active range of motion exercises
Late Phase
- Wobble board training
- Advanced proprioception
Return to Sport
- Approximately 3 months
- Based on functional stability
Failure of Conservative Treatment
When to Consider
- After 6 months of structured rehabilitation
High-Risk Groups
- Athletes
- Persistent instability
Surgical Management
Options
1. Anatomic Repair (Preferred)
Gold Standard
Broström–Gould Procedure
- Repair ATFL and CFL
- Reinforcement using extensor retinaculum
Outcomes
- Success rate: 80–90%
2. Non-Anatomic Reconstruction
Example
- Chrisman–Snook procedure
Disadvantages
- Stiffness
- Subtalar arthritis
- Altered biomechanics
3. Arthroscopy-Assisted Procedures
Role
- Detects intra-articular pathology in ~80%
Associated Findings
- Loose bodies
- Osteochondral lesions
- Synovitis
Recent Advances
Internal Brace Augmentation
- Fiber tape reinforcement
- Faster return to sport
- Approximately 80% return by 6 months
Adjunct Procedures
- Microfracture
- Loose body removal
- AMIC (cartilage repair)
Deltoid Ligament Injury
Characteristics
- Rarely isolated
Common Associations
- Syndesmotic injury
- Weber C fractures
- Flatfoot / posterior tibial dysfunction
Management
- Treat associated pathology
- Repair if persistent symptoms
Complications if Untreated
- Chronic pain
- Persistent instability
- Osteoarthritis
Deformities
- Varus deformity (lateral injury)
- Valgus deformity (medial injury)
Key Take-Home Points
- Lateral ligament complex is most commonly involved
- Differentiate functional vs mechanical instability
- Rehabilitation is first-line treatment
- Surgery indicated after failed conservative management
- Broström–Gould procedure remains the gold standard
- Arthroscopy helps identify associated intra-articular pathology

Leave a Reply