Courtesy: Vijay Shetty, Hiranandani Hospital, Mumbai, India
Introduction
Platelet-Rich Plasma (PRP) is widely used in sports medicine and orthopaedics.
It has gained popularity due to its applications in:
- Cosmetic medicine
- Hair restoration
- Sports injury management
Objectives
This overview aims to explain:
- What PRP is
- Its biological mechanism
- Current evidence
- Practical clinical application
Platelet Biology
Platelet Characteristics
- Approximately 250 million platelets per mL of blood
- Contain intracellular granules rich in:
- Growth factors
- Cytokines
- Bioactive proteins
Biological Functions
Platelets play a role in:
- Hemostasis
- Immune modulation
- Tissue repair
- Inflammation regulation
- Maintenance of homeostasis
Historical Evolution of PRP
- 1940s – Discovery of growth factors
- 1980s – Use in wound healing
- 1990s – Application in maxillofacial surgery
- Early 2000s ? Adoption in orthopaedics
Early techniques included autologous clot use in meniscal repair.
Definition of PRP
PRP is defined as:
Autologous plasma with platelet concentration higher than baseline
Evolution of Definition
- Earlier: 3–5× baseline platelet concentration
- Current: Any concentration above baseline
PRP Preparation
Basic Steps
- Blood collection
- Centrifugation
- Plasma separation
- Platelet concentration
- Injection into target tissue
Variability in Preparation
PRP systems differ in:
- Centrifugation protocols
- Platelet concentration
- Leukocyte content
- Final volume
Key Issue: Lack of standardization makes studies difficult to compare.
Platelet Growth Factors
Key components include:
- PDGF (Platelet-derived growth factor)
- TGF- (Transforming growth factor)
- VEGF (Vascular endothelial growth factor)
- EGF (Epidermal growth factor)
- IGF (Insulin-like growth factor)
Biological Effects
- Cell proliferation
- Angiogenesis
- Tissue healing
- Regulation of inflammation
Biological Variability
Platelet concentration varies due to:
- Time of day
- Individual physiology
- Health status
This contributes to inconsistent clinical outcomes.
Types of PRP
Leukocyte-Rich PRP
- High white cell content
- Strong inflammatory response
- Previously used for tendon healing
Leukocyte-Poor PRP
- Lower inflammatory response
- Preferred for:
- Intra-articular injections
- Most clinical indications
PRP Activation
Platelets release growth factors upon activation.
Methods
- Chemical
- Mechanical
- Natural activation after injection
Current practice commonly relies on natural activation in tissues
PRP Preparation Systems
Regen System
- Requires 8–9 mL blood
- Single-spin centrifugation
- Produces ~5 mL PRP
Advantages
- Quick
- Office-based
- Minimal blood requirement
EmCyte M-Site System
- Double-spin technique
- Requires ~60 mL blood
- Produces higher platelet concentration
Procedure Time
- ~40–45 minutes
PRP Injection Technique
General Principles
- Knee injections may be performed without imaging
- Tendon/small joint injections –Prefer:
- Ultrasound
- Fluoroscopy
- CT guidance
Pre-Injection Considerations
- Aspirate joint effusion
- Avoid mixing PRP with local anesthetics
Local anesthetics may reduce platelet activity
Platelet Dose and Outcomes
Findings from Studies
- Higher platelet concentration — Better outcomes
Observed Data
- Positive studies: ~5.5 billion platelets
- Negative studies: ~2.3 billion platelets
Evidence remains inconsistent
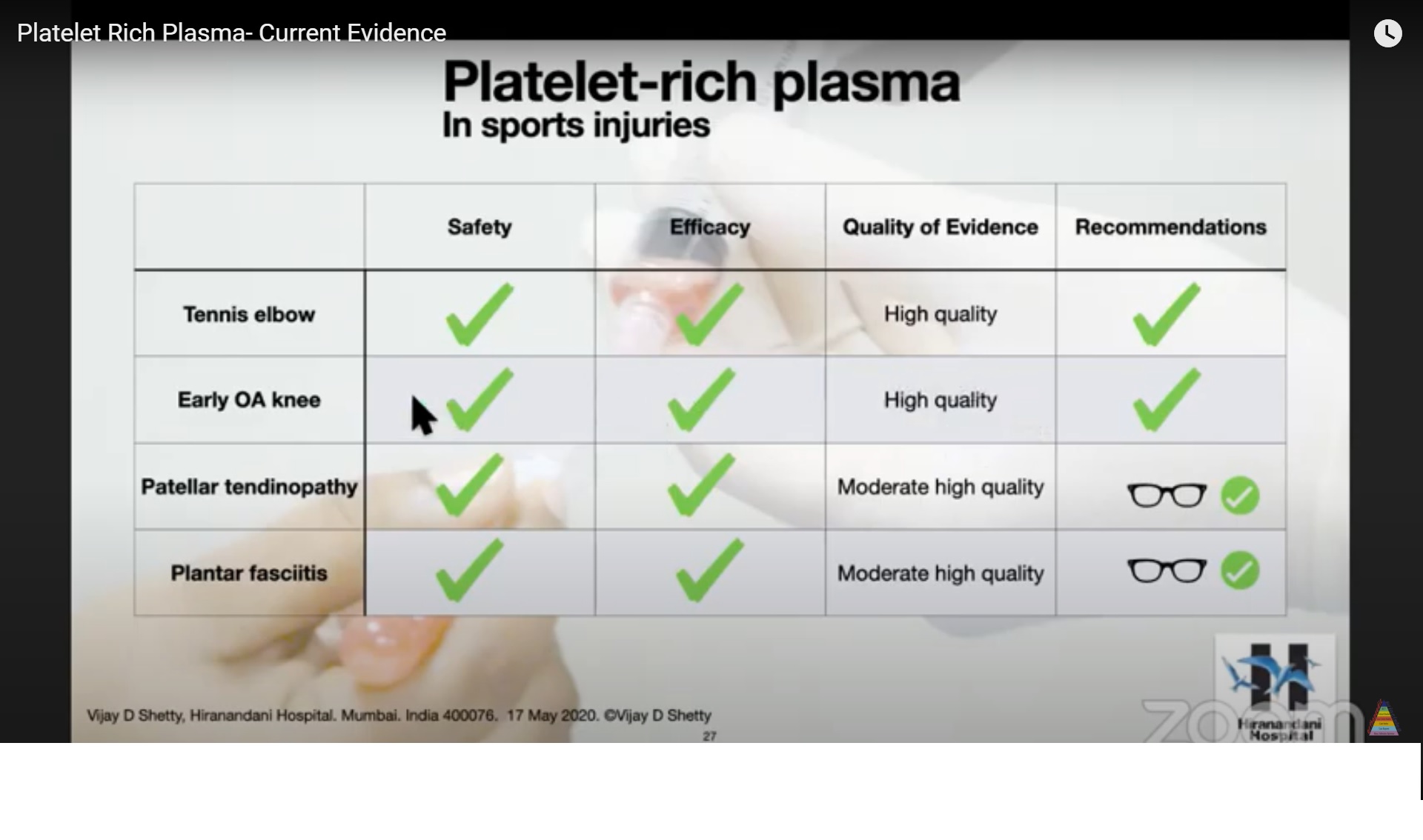
Clinical Applications of PRP
1. Lateral Epicondylitis
- Most common indication
- Shows small but significant improvement
2. Rotator Cuff Tears
- Limited benefit when used alone
- Better outcomes as adjunct during surgery
3. Knee Osteoarthritis
Comparative Effect Duration
| Treatment | Duration |
|---|---|
| Corticosteroid | 6–12 weeks |
| Hyaluronic acid | 6–8 months |
| PRP | Up to 12 months |
Key Insight
- PRP often:
- Superior to corticosteroids
- Slightly better than hyaluronic acid
4. Early Cartilage Degeneration
Effects
- Reduces inflammation
- Improves cartilage metabolism
- Provides symptom relief
PRP is reparative, not truly regenerative
5. Muscle Injuries (e.g., Hamstring)
- No clear benefit over standard rehabilitation
Safety Profile
PRP is considered very safe:
Advantages
- Autologous (no immune reaction)
- Minimal infection risk
- No systemic side effects
- No cartilage toxicity
Post-Injection Protocol
NSAID Restrictions
- Avoid:
- 1 week before injection
- 3–7 days after injection
NSAIDs inhibit platelet function
Pain Control
- Use paracetamol (acetaminophen)
Activity Recommendations
- Relative rest for a few days
- Gradual return to activity
Examples
- Boot – Achilles tendinopathy
- Brace – Patellar tendon injury
Clinical Outcomes
- 70–80% patients show improvement
- Onset: 2–6 weeks
No improvement by 6 weeks – unlikely to benefit further
Emerging Research
Current Focus Areas
- Proteomic analysis of PRP
- Identification of active proteins (e.g., platelet factor-4)
- Role in anti-aging and neurodegeneration
Experimental Findings
- PRP may influence:
- Cellular aging
- Tissue repair pathways
Future Directions
Potential developments include:
- Freeze-dried platelet preparations
- Standardized PRP formulations
- Targeted growth factor therapies
Key Take-Home Messages
- PRP is a widely used orthobiologic therapy
- It involves injection of concentrated autologous platelets
Best-Supported Indications
- Knee osteoarthritis
- Lateral epicondylitis
- Selected tendon disorders
Major Limitations
- Lack of standardization
- Variable platelet composition
- Heterogeneous clinical evidence
Final Conclusion
PRP is a safe and promising treatment, but:
- Evidence remains inconsistent
- High-quality research is still needed


Good