Courtesy Dr Jefferey Yao, Dr Ashok Shyam, Ortho TV
Basic Wrist Ligament Anatomy
- Wrist ligaments act as static stabilizers that guide and constrain motion of the carpus.
- Wrist ligaments are classified into two main groups:
Intrinsic Ligaments
- Located entirely within the carpal bones.
- Connect adjacent carpal bones.
- Example:
- Scapholunate ligament
- Lunotriquetral ligament
Extrinsic Ligaments
- Connect carpal bones to the radius or ulna.
- Cross either:
- Radiocarpal joint
- Midcarpal joint
Concept of Carpal Instability
- Malalignment does not necessarily equal instability.
- Some individuals (e.g., ligamentous laxity) may show radiographic malalignment but remain asymptomatic.
True Carpal Instability
Defined as:
- Abnormal load transfer across the carpal joint
- Abnormal motion between carpal bones
- Associated pain and functional impairment
Classification of Carpal Instability (Mayfield Concept)
Carpal instability is classified as:
- Carpal Instability Dissociative (CID)
- Instability within a carpal row
- Example:
- Scapholunate dissociation
- Carpal Instability Non-Dissociative (CIND)
- Instability between proximal and distal carpal rows
- Carpal Instability Complex (CIC)
- Combination of CID and CIND
- Seen in perilunate dislocations
Perilunate Injuries
- Represent a spectrum of carpal instability injuries.
- Usually occur due to high-energy trauma.
Common Mechanisms
- Motorcycle accidents
- Falls from height
- Falls from ladders or scaffolds
Mechanism of Injury
- Forceful wrist hyperextension
- Ulnar deviation
- Carpal supination
Mayfield Classification of Perilunate Instability
Describes progressive ligament injury around the lunate.
Stage I
- Scapholunate ligament rupture
- In greater arc injuries:
- Scaphoid fracture
Stage II
- Injury progresses through capitolunate joint
- May include:
- Capitate dislocation
- Capitate fracture
Stage III
- Additional injury to:
- Lunotriquetral ligament
- Lunate remains in the lunate fossa
Stage IV
- Complete lunate dislocation
- Lunate displaced volarly into the carpal tunnel
Types of Perilunate Injuries
Lesser Arc Injuries
- Pure ligamentous injuries
- No associated fractures
Greater Arc Injuries
- Include fractures of carpal bones
- Examples:
- Scaphoid
- Capitate
- Triquetrum
- Radial styloid
Radiographic Diagnosis
Perilunate injuries are commonly missed on wrist X-rays.
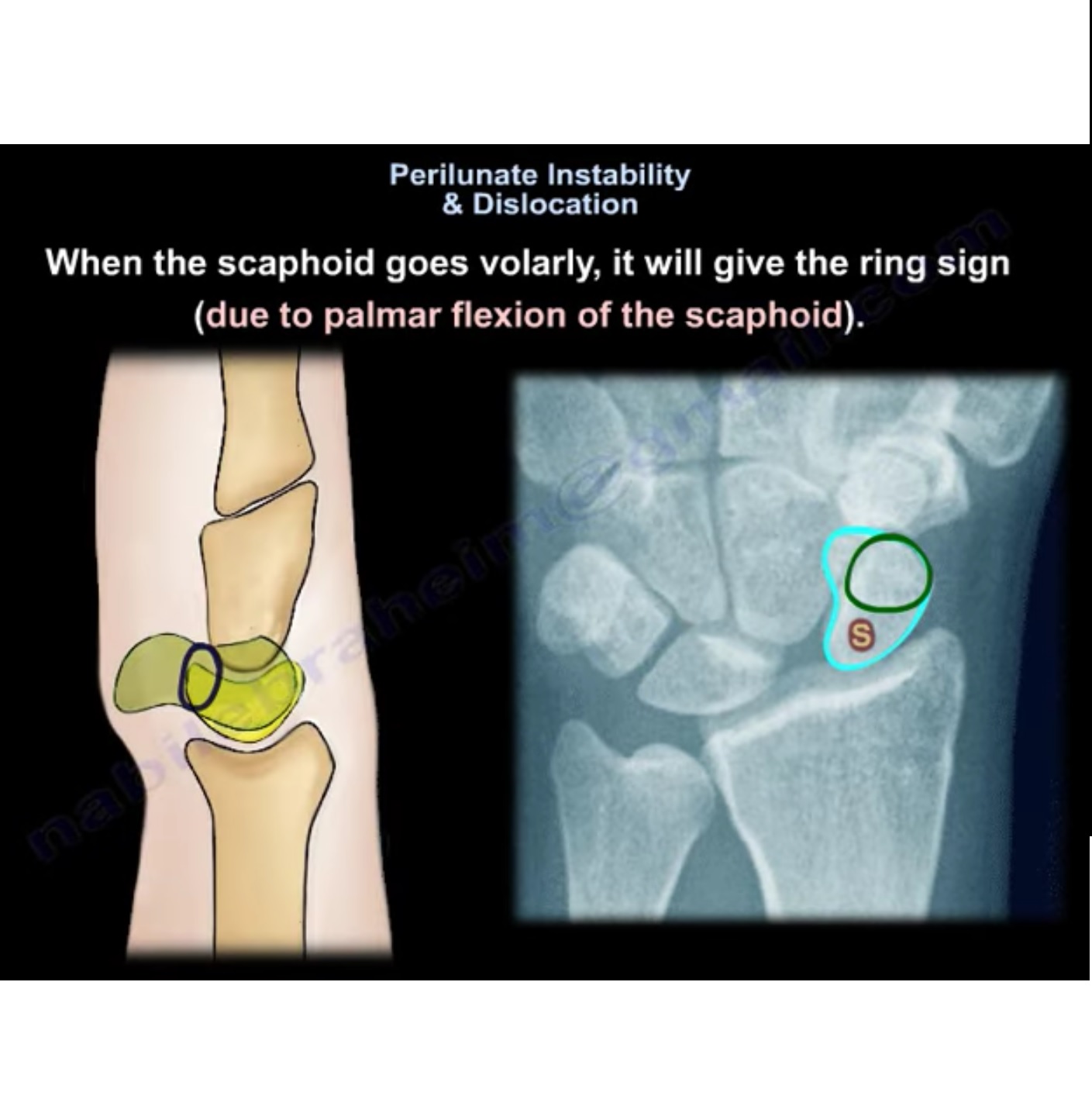
PA View Findings
- Loss of Gilula’s arcs
- Triangular-shaped lunate (instead of trapezoidal)
- Known as the “piece-of-pie sign.”
Lateral View Findings
- Volar displacement of lunate
- Known as the “spilled teacup sign.”
Reverse Perilunate Injury
- Injury progression begins ulnar side first.
- Starts with lunotriquetral ligament rupture.
- Progresses counterclockwise toward the scapholunate side.
Initial Management
- Median Nerve Assessment
- Median nerve compression is common due to lunate displacement into the carpal tunnel.
- Closed Reduction (Emergency)
Performed under adequate sedation.
Reduction steps:
- Apply longitudinal traction
- Hyperextend wrist
- Stabilize lunate with thumb
- Gradually bring wrist into flexion
- Capitate reduces back into alignment with lunate
Definitive Treatment
Most cases require early surgical stabilization.
Options
Arthroscopic Management
- Reduction
- Percutaneous pinning
- Capsular repair
Advantages:
- Less soft tissue disruption
- Preservation of blood supply
- Less scar formation
- Allows evaluation of associated injuries
Open Reduction and Internal Fixation
Approaches include:
Dorsal Approach
- Access to dorsal scapholunate ligament
- Most important stabilizing component
Volar Approach
- Access to:
- Volar lunotriquetral ligament
- Volar capsule
- Allows median nerve decompression
Combined Dorsal + Volar Approach
- Used for severe or complex injuries
Arthroscopic Ligament Repair
Example technique:
- Arthroscopic capsuloligamentous repair
- Sutures passed through ligament
- Tied externally
- Knot pushed back into joint
Advantages:
- Minimally invasive
- Good stabilization of scapholunate interval
Treatment of Advanced Perilunate Injuries
Stage III or IV Injuries
Often treated with:
- Open reduction
- Ligament repair using suture anchors
- Temporary fixation with K-wires or screws
Temporary Screw Fixation
Alternative to K-wire fixation.
Advantages:
- Allows early wrist mobilization
- Screws typically removed after ~3 months
Perilunate Fracture Dislocations (Greater Arc Injuries)
Examples include:
Trans-Scaphoid Perilunate Dislocation
Treatment:
- Scaphoid fixation (screw)
- Ligament stabilization
Trans-Capitate Perilunate Dislocation
Treatment:
- Capitate fixation
- Carpal stabilization
Trans-Radial Styloid Perilunate Injury
Treatment:
- Radial styloid fixation
- Carpal realignment
Complications
Early Complications
Missed Diagnosis
- One of the most common complications
Median Neuropathy
- Often improves after reduction
- Persistent symptoms ? urgent carpal tunnel release
Avascular Necrosis (AVN)
May affect:
- Scaphoid
- Lunate
However:
- True AVN is relatively uncommon if ligaments remain attached.
Late Complications
Carpal Instability
- Persistent ligament injury may lead to:
- Scapholunate instability
- Chronic carpal instability
Post-traumatic Arthritis
- Occurs in >50% of patients long term.
Salvage Procedures
Used for chronic or missed injuries.
Options include:
- Proximal row carpectomy
- Limited wrist fusion
- Total wrist arthrodesis
Key Points
- Perilunate injuries are high-energy wrist injuries.
- They are frequently missed on initial radiographs.
- Diagnosis requires careful evaluation of:
- Gilula’s lines
- Lunate alignment
- Early management includes:
- Urgent closed reduction
- Median nerve assessment
- Early surgical stabilization is usually required.
- Delay beyond 3 months often necessitates salvage procedures.


Leave a Reply