Courtesy: Amr Abdelgawad, Maimonaides Medical Centre, Brooklyn, NewYork, USA
Iliac Crest Bone Graft Harvesting
- Bone graft can be harvested from anterior or posterior iliac crest.
- Anterior iliac crest: structure at greatest risk is the lateral femoral cutaneous nerve.
- Lateral femoral cutaneous nerve lies approximately 2–3 cm medial to the ASIS.
- Posterior iliac crest graft: cluneal nerves at risk (?8 cm lateral to PSIS).
- Distal extension may risk injury to superior gluteal neurovascular bundle.
Ilioinguinal Approach
- Commonly used for acetabular fractures involving anterior column.
- Key structure: iliopectineal fascia.
- This fascia separates iliopsoas muscle and femoral nerve (laterally) from iliac vessels (medially).
- Fascia must be released to access the true pelvis.
Anterior Intrapelvic (Stoppa) Approach
- Provides excellent access to quadrilateral plate.
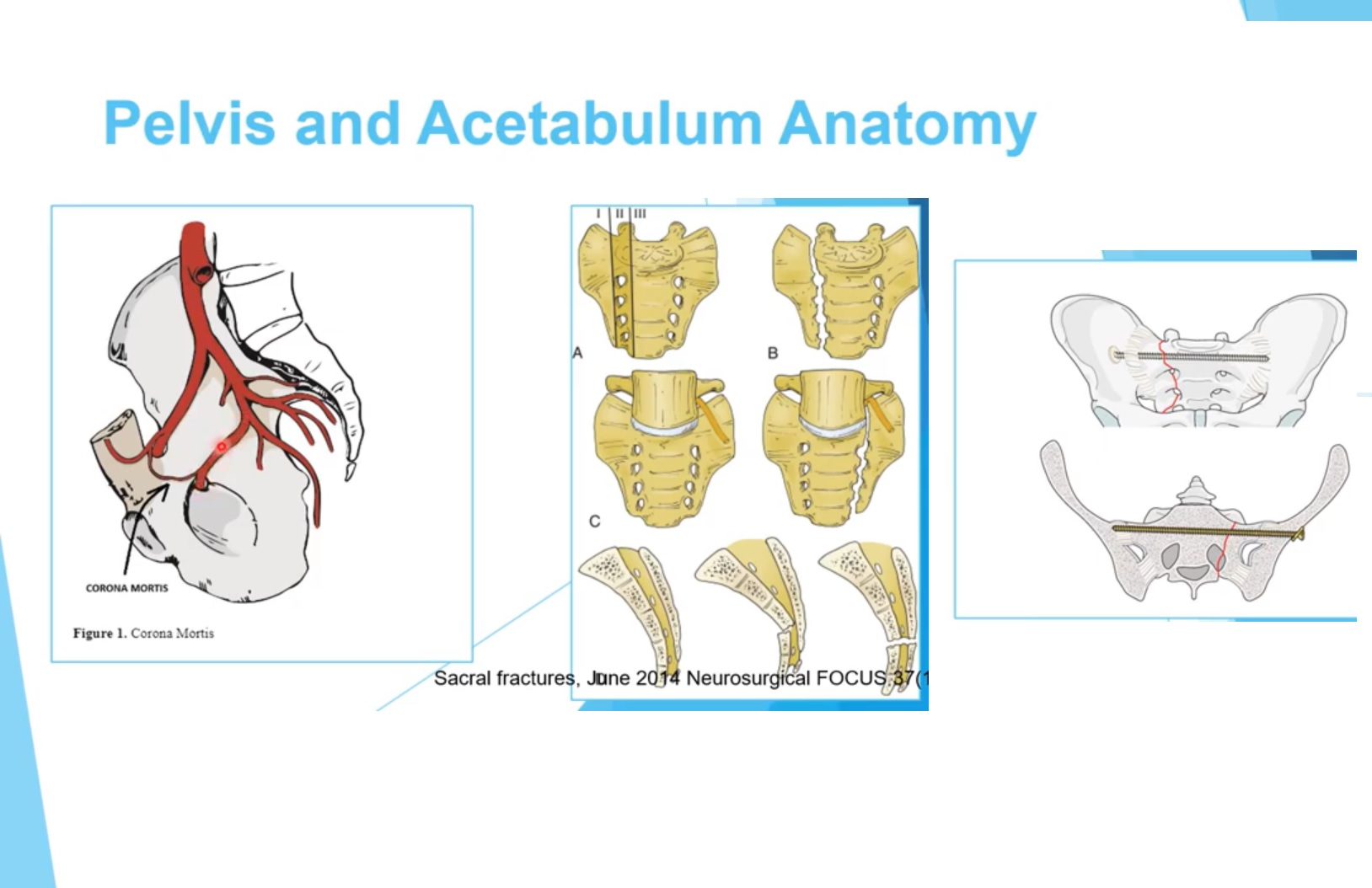
- Important structure at risk: corona mortis.
- Corona mortis is an anastomosis between external iliac/inferior epigastric vessels and obturator vessels.
- Located approximately 6 cm lateral to the pubic symphysis.
Hip Surgical Approaches
- Smith-Petersen (anterior) approach.
- Watson-Jones (anterolateral) approach.
- Hardinge (direct lateral) approach.
- Posterior approach through gluteus maximus.
Smith-Petersen (Anterior) Approach
- Interval between sartorius and tensor fascia lata.
- Sartorius supplied by femoral nerve.
- Tensor fascia lata supplied by superior gluteal nerve.
- This is the only true interneural approach to the hip.
- Structures at risk: lateral femoral cutaneous nerve and ascending branch of lateral femoral circumflex artery.
Watson-Jones (Anterolateral) Approach
- Interval between tensor fascia lata and gluteus medius.
- Not a true interneural plane because both muscles are supplied by the superior gluteal nerve.
Direct Lateral (Hardinge) Approach
- Approach splits the gluteus medius.
- Do not extend more than 5 cm proximal to greater trochanter.
- Risk of injury to superior gluteal nerve.
- Hip dislocation occurs anteriorly in this approach.
Posterior Hip Approach
- Approach through gluteus maximus.
- Gluteus maximus supplied by inferior gluteal nerve.
- Short external rotators (piriformis, obturator internus, gemelli) released.
- Associated with higher risk of postoperative dislocation.
Hip Arthroscopy Portals
- Posterolateral portal close to sciatic nerve.
- Internal rotation of hip moves femur away from sciatic nerve to reduce risk.
- Anterior portal close to lateral femoral cutaneous nerve and ascending branch of lateral femoral circumflex artery.
- Anterolateral portal close to superior gluteal vessels.
Surgical Hip Dislocation – Trochanteric Osteotomy
- Used to safely dislocate hip without compromising blood supply.
- Blood supply mainly from medial femoral circumflex artery.
- Trochanteric osteotomy keeps piriformis and external rotators intact.
- Osteotomy typically 1–1.5 cm thick.
- Z-shaped capsulotomy performed to preserve vascular supply.
Blood Supply of Femoral Head
- Main supply: deep branch of medial femoral circumflex artery.
- Artery arises from profunda femoris artery.
- Passes between pectineus and iliopsoas muscles.
- Travels posteriorly along quadratus femoris.
- Then runs beneath obturator externus and external rotators before entering capsule.
- Inferior gluteal artery may contribute in some individuals.
Greater and Lesser Sciatic Notch Anatomy
- Separated by sacrospinous ligament.
- Lesser sciatic notch contains obturator internus and gemelli muscles.
- Greater sciatic notch contains piriformis muscle.
Structures Above and Below Piriformis
- Above piriformis: superior gluteal nerve and artery.
- Below piriformis: sciatic nerve, inferior gluteal nerve and artery.
- Also below piriformis: pudendal nerve, internal pudendal artery, nerve to obturator internus, nerve to quadratus femoris.
L5 Nerve Root in Pelvic Fixation
- L5 root passes anterior to sacral ala.
- Anteriorly placed iliosacral screws may injure L5 root.
- L5 root lies about 2 cm from sacroiliac joint.
- Screws should not extend more than ~1.5 cm anterior to SI joint.
Acetabular Teardrop
- Radiographic landmark used in acetabular fractures and total hip arthroplasty.
- Represents bone between cotyloid fossa and quadrilateral plate.
Pelvic Teardrop Corridor
- Used for anterior external fixation pins.
- Corridor between AIIS and PSIS.
- Best visualized on obturator outlet view.
Hip Joint Biomechanics
- Hip is a ball-and-socket joint.
- Allows three degrees of freedom: flexion/extension, abduction/adduction, rotation.
- Does not allow translation.
- Maximum joint pressure occurs in extension and internal rotation.
- Patients with effusion prefer flexion and external rotation.
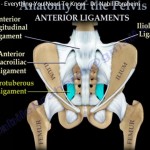
Hip Ligaments
- Iliofemoral ligament (Y ligament of Bigelow) – strongest ligament in body.
- Extends from AIIS to intertrochanteric line.
- Pubofemoral ligament – from pubis to femur.
- Ischiofemoral ligament – from ischium to femur.
- Ischiofemoral ligament limits internal rotation.
Femoral Triangle
- Borders: inguinal ligament (superior), sartorius (lateral), adductor longus (medial).
- Floor: iliopsoas, pectineus, adductor longus.
- Contents (lateral to medial): femoral nerve, femoral artery, femoral vein, deep inguinal lymph node.
- Femoral nerve lies outside femoral sheath.
Leave a Reply