Courtesy Dr Frank Noyes, Dr Ashok Shyam, Ortho TV
PCL and Posterolateral Corner Injuries
Overview
Posterior cruciate ligament (PCL) injuries are less common than ACL injuries but are often more technically demanding to diagnose and treat. These injuries frequently occur following high-energy trauma and are commonly associated with multiligament knee injuries.
Associated injuries may include:
- PCL + MCL injury
- PCL + posterolateral corner (PLC) injury
- PCL + ACL injury
- Knee dislocations
Mechanism of Injury
Common Mechanisms
The classic mechanism involves:
- Direct anterior blow to the tibia causing posterior tibial displacement
Common causes include:
- Sports-related contact injuries
- Road traffic accidents
- Motorcycle accidents
Initial Assessment
Rule Out Neurovascular Injury
The first and most important step is evaluation for vascular injury, particularly involving the popliteal artery.
Posterior tibial displacement can stretch vascular structures and cause:
- Immediate vascular compromise
- Delayed vascular injury
Important Principles
- Frequent neurovascular monitoring is essential
- Early vascular surgery involvement may be required
- Knee dislocations should always be considered limb-threatening injuries
PCL Anatomy
Structural Components
The PCL is the largest ligament in the knee and consists of:
- Anteromedial bundle
- Posterolateral bundle
Associated structures include:
- Ligament of Wrisberg
- Ligament of Humphrey
Function
The PCL primarily functions to:
- Prevent posterior tibial translation
- Stabilize the knee during flexion
Non-Operative Management of Isolated PCL Tears
Why Conservative Treatment Works
Compared to the ACL, the PCL has:
- Better vascularity
- Greater healing potential
Many isolated PCL injuries can heal satisfactorily without surgery.
Treatment Principles
The key objective is maintaining the tibia in an anteriorly reduced position while healing occurs.
Methods
- Posterior support brace
- Cast with posterior padding
- Prevention of posterior sag
Typical Protocol
- Immobilization for approximately 4 weeks
- Controlled rehabilitation afterward
Outcomes
Possible healing outcomes include:
- Complete healing
- Partial healing with mild posterior laxity
- Functional stability despite residual laxity
Posterior laxity less than approximately 6 mm may still allow good function without surgery.
Indications for Surgery
Surgical reconstruction is generally indicated for:
- Posterior translation greater than 10–12 mm
- Persistent instability
- Difficulty with deceleration activities
- Instability while walking downhill
- Combined ligament injuries
Graft Considerations in PCL Reconstruction
Single-Bundle vs Double-Bundle Reconstruction
Double-Bundle Reconstruction
Advantages:
- More anatomical
Disadvantages:
- Technically demanding
Current Trend
Many surgeons now prefer:
- Large single-bundle graft reconstruction
This can adequately cover approximately 60–70% of the native footprint and provides satisfactory clinical outcomes.
Graft Options
Common graft choices include:
Quadriceps Tendon Autograft
Often preferred in athletes because of:
- Large graft diameter
- Strong fixation potential
Achilles Tendon Allograft
Useful especially in:
- Multiligament reconstructions
Allografts
Advantages:
- Reduced donor-site morbidity
- Useful when multiple grafts are required
Bone–Patellar Tendon–Bone Graft
Usually considered too small for isolated PCL reconstruction.
Surgical Technique of PCL Reconstruction
Modern Techniques
Current approaches commonly use:
- All-inside arthroscopic reconstruction
Older open posterior approaches are now less frequently used.
Technical Challenges
Neurovascular Risk
One of the greatest technical concerns is the proximity of the popliteal neurovascular structures.
Important point:
- Neurovascular structures may lie only 4–5 mm from the tibial tunnel
This creates significant risk during tunnel preparation.
Instrumentation
Specialized instrumentation improves safety and accuracy.
Common tools include:
- Curved instruments for posterior access
- Safety drill guides
- Posterior arthroscopic portals
- Flip-cutter systems
Tibial Tunnel Placement
Landmark
The tibial tunnel is placed near the:
- “Teardrop” area of the posterior tibia
Key Precautions
- Avoid drilling below the teardrop
- Avoid posterior capsule violation
- Use controlled drilling techniques
Femoral Tunnel Placement
Goal
- Restore anatomic femoral footprint coverage
Common Techniques
- Outside-in drilling
- Flip-cutter technique
The flip-cutter technique has become increasingly popular because it simplifies tunnel creation.
Graft Fixation
Femoral Side
Commonly uses:
- Suspensory fixation
- Button systems
Tibial Side
Usually fixed with:
- Interference screw fixation
Rehabilitation After PCL Reconstruction
Key Principles
Rehabilitation is critical for successful outcomes.
Important Goals
- Prevent posterior sag
- Protect graft healing
- Restore controlled motion
Early Rehabilitation Precautions
Avoid Early Hamstring Activation
Hamstring contraction increases posterior tibial translation and may stress the graft.
Bracing
Braces should maintain:
- Anterior tibial support
Motion
- Early controlled range of motion is encouraged
- Excessive stress should be avoided
Posterolateral Corner (PLC) Injuries
Importance
PLC injuries commonly accompany PCL injuries and must be recognized and treated appropriately.
Failure to address PLC instability can lead to:
- Persistent instability
- PCL graft failure
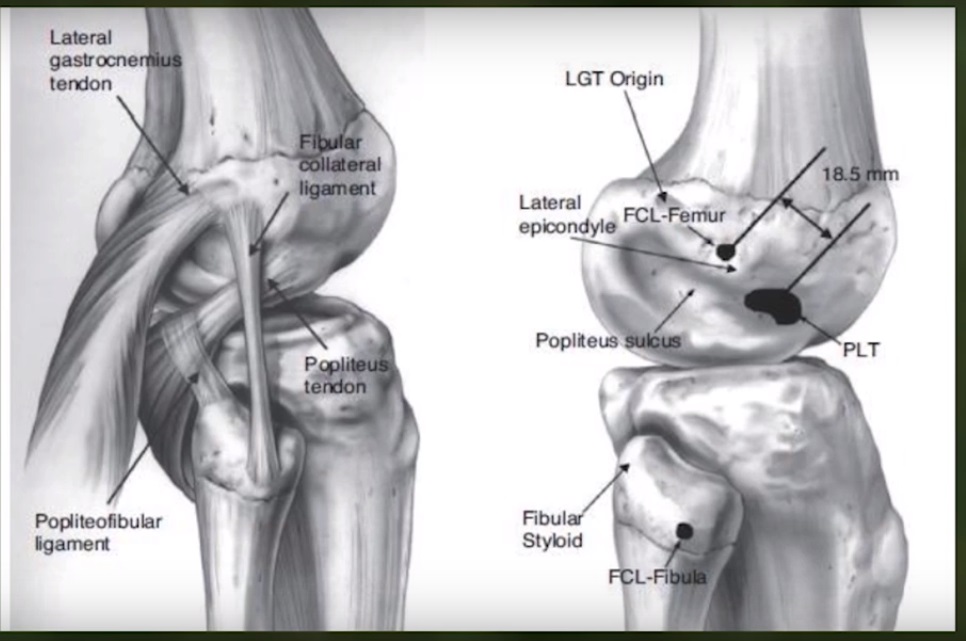
Structures Involved in PLC Injuries
Key structures include:
- Fibular collateral ligament (LCL)
- Popliteus tendon
- Posterior capsule
Management of PLC Injuries
Acute Injuries
Typically treated with:
- Repair plus reconstruction
Common strategy:
- Single graft spanning fibula to femur
Chronic PLC Injuries
Usually require formal reconstruction using:
- Achilles tendon allograft
- Bone–tendon–bone grafts
Posterolateral Advancement
Indication
- Stretch injuries without complete rupture
Technique
Existing posterolateral structures are advanced and tightened.
Most commonly used in:
- Chronic laxity situations
Surgical Principles in PLC Reconstruction
Protect the Common Peroneal Nerve
Identification and protection of the nerve are mandatory during surgery.
Goals of Reconstruction
- Restore lateral stability
- Prevent hyperextension instability
Rehabilitation After PLC Reconstruction
Rehabilitation following PLC surgery is generally more cautious than ACL rehabilitation.
Common Strategies
- Rigid immobilization initially
- Bivalve cast or brace
- Supervised controlled motion progression
Key Takeaways
- Always rule out vascular injury first
- Many isolated PCL tears heal successfully without surgery
- Surgery is indicated for significant instability or combined injuries
- PCL reconstruction is technically demanding
- Proper tunnel placement is critical
- PLC injuries must be treated to prevent graft failure
- Rehabilitation plays a major role in final outcome


Leave a Reply