Courtesy Dr Brett Fritsch, Dr Ashok Shyam, Ortho TV
Posterolateral Corner (PLC) Injuries
Overview
The posterolateral corner (PLC) of the knee is a complex anatomical region consisting of multiple stabilizing structures. Historically, PLC injuries were considered difficult to diagnose and associated with poor outcomes. Improved understanding of anatomy, biomechanics, and reconstruction techniques has significantly improved results.
PLC injuries are commonly associated with:
- Multiligament knee injuries
- Knee dislocations
- High-energy trauma
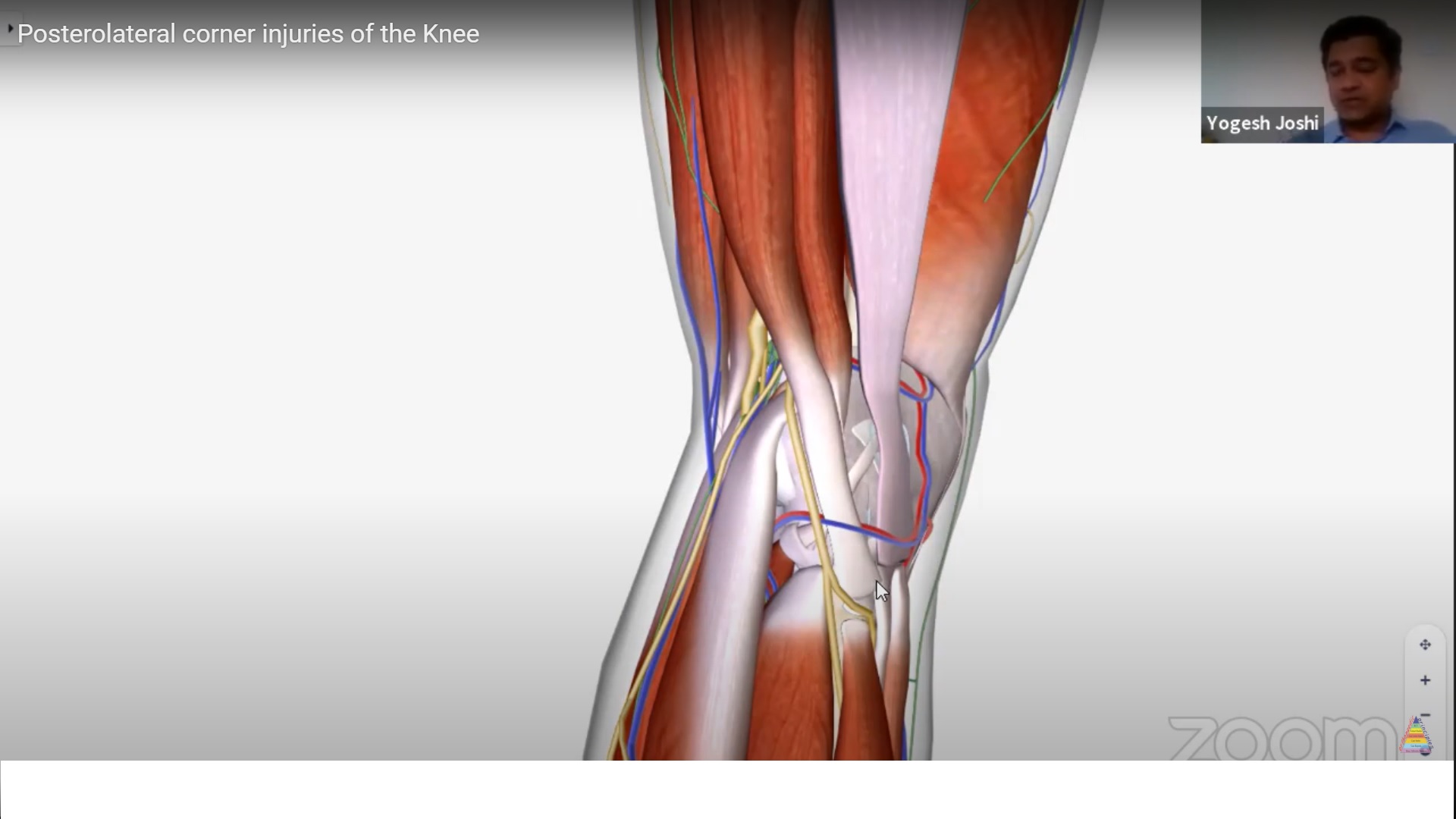
Functional Anatomy of the PLC
Important Structures
The clinically important structures of the PLC include:
- Lateral collateral ligament (LCL)
- Popliteus tendon
- Popliteofibular ligament
- Biceps femoris
- Iliotibial band
- Posterolateral capsule
- Lateral meniscus
- Common peroneal nerve
Functions of the PLC
The PLC acts as the primary restraint to:
- Varus stress
- External rotation
It also works synergistically with:
- ACL
- PCL
Deficiency of the PLC can therefore compromise cruciate ligament stability and reconstruction outcomes.
Classification of PLC Injuries
PLC injuries are broadly classified into:
Acute Injuries
- Recent traumatic injuries
- Usually associated with high-energy trauma
Chronic Injuries
- Delayed or missed diagnosis
- Persistent instability and gait abnormalities
Acute PLC Injuries
Mechanism of Injury
Common mechanisms include:
- Road traffic accidents
- Sports injuries
- Knee dislocations
Road traffic accidents account for approximately 50% of severe PLC injuries.
Associated Injuries
Systemic Injuries
Acute PLC injuries may occur with:
- Spine injuries
- Chest trauma
- Long bone fractures
Local Knee Injuries
Common associated knee injuries include:
- Meniscal tears
- Tibial plateau fractures
- Neurovascular injuries
- Multiligament injuries
Initial Management Priorities
Trauma Principles
Management begins with:
- ATLS / EMST protocols
- Stabilization of life-threatening injuries
Vascular Assessment
Importance
The popliteal artery is at risk in PLC injuries and knee dislocations.
Failure to identify vascular injury can result in limb-threatening complications.
Assessment Methods
Evaluation includes:
- Pulse examination
- Ankle–brachial index (ABI)
- Doppler ultrasound
- CT angiography
Vascular Assessment Algorithm
If Knee Dislocation Present
- Reduce the knee immediately
If Limb Ischemia Present
- Urgent angiography required
If Pulses Are Asymmetric
- Perform CT angiography
If Pulses Are Normal
- ABI < 0.9 ? CT angiography
- ABI > 0.9 ? serial monitoring
Neurological Assessment
Common Peroneal Nerve
Peroneal nerve injury may occur in up to 25% of PLC injuries.
Examination includes:
- Dorsiflexion
- Foot eversion
- Sensation over dorsum of foot
Tibial Nerve Examination
Assess:
- Plantarflexion
- Sole sensation
Stabilization of Acute Injuries
Reduction
Usually achieved with:
- Gentle traction
Immobilization Options
- Hinged brace
- Splint
- Plaster slab
Severe Instability
May require:
- External fixation
Diagnosis of PLC Injuries
Diagnosis Relies On
- History
- Clinical examination
- Imaging
Imaging
X-rays
Useful for identifying:
- Fibular head avulsion fractures
MRI
Best imaging modality in acute injuries.
MRI evaluates:
- Ligament injury
- Meniscal pathology
- Associated cruciate injuries
CT Scan
Useful when fractures are suspected.
Chronic PLC Injuries
Challenges
Diagnosis of chronic PLC injuries is more difficult because:
- MRI findings may appear normal
- Instability becomes subtle
- Compensatory gait develops
Important Diagnostic Tools
- Detailed clinical examination
- Stress radiographs
- Gait analysis
Clinical Examination Tests
1. Varus Stress Test
At 30°
- Isolates the LCL
At 0°
- Suggests combined ligament injury
2. Dial Test
Performed at:
- 30°
- 90° knee flexion
Interpretation
- Increased external rotation at 30° only ? PLC injury
- Increased external rotation at both 30° and 90° ? PLC + PCL injury
3. External Rotation Recurvatum Test
Assesses:
- Heel elevation asymmetry
- Hyperextension instability
4. External Rotation Posterior Drawer Test
Posterior and external rotational force is applied to evaluate combined instability.
5. Reverse Pivot Shift Test
Posterolateral tibial subluxation reduces during extension.
Important point:
- Compare with contralateral side because specificity is limited.
6. Gait Analysis
Look for:
- Varus thrust
- Hyperextension gait
Stress Radiographs
Stress radiographs are especially valuable in chronic injuries.
Interpretation
- 2 mm opening ? isolated LCL injury
- 4 mm opening ? Grade III PLC injury
Principles of Management
Evidence-Based Concepts
Studies suggest:
- Surgery is superior to non-operative treatment
- Early surgery is superior to delayed surgery
- Reconstruction plus repair is superior to repair alone
Timing of Surgery
Ideal Timing
Optimal timing is approximately:
- Day 7–14 after injury
- Around Day 10 is often preferred
Advantages include:
- Easier dissection
- Better tissue quality
- Less scarring
Repair vs Reconstruction
Repair Alone
Associated with:
- High failure rates (~40%)
Reconstruction Plus Repair
Provides:
- Better stability
- Improved long-term outcomes
Success Rates
Reconstruction
Approximately:
- 90% success rate
Repair Alone
Approximately:
- 60% success rate
Surgical Techniques
Structures Typically Reconstructed
- LCL
- Popliteus tendon
- Popliteofibular ligament
Reconstruction Techniques
Grade II Injuries
Usually treated with:
- Fibular-based reconstruction
Grade III Injuries
Require:
- Tibia + fibula-based reconstruction
- More anatomical restoration
Surgical Approach
Posterolateral Approach
Typically involves three windows:
Window 1
- Posterior to biceps femoris
- Accesses fibula and peroneal nerve
Window 2
- Between biceps femoris and IT band
- Accesses posterolateral capsule
Window 3
- Through IT band
- Accesses femoral insertion sites
Common Peroneal Nerve Protection
Identification and protection of the common peroneal nerve is mandatory during surgery.
Graft Choices
Autografts
Generally preferred.
Allografts
Acceptable if properly prepared.
Synthetic Augmentation
Emerging role, though long-term evidence remains limited.
Chronic PLC Injury Considerations
Alignment Assessment
Evaluate for:
- Varus malalignment
Persistent varus overload may compromise reconstruction.
Role of Osteotomy
In chronic cases:
- Osteotomy may be required
- Sometimes osteotomy alone improves symptoms
- Often combined with PLC reconstruction
Outcomes
Reported outcomes after reconstruction include:
- Lysholm scores approximately 85–90
- IKDC scores approximately 75–85
Better outcomes occur with:
- Reconstruction plus repair
- Proper alignment correction
Acute vs Chronic PLC Injuries
| Feature | Acute Injury | Chronic Injury |
|---|---|---|
| Diagnostic difficulty | Easier | More difficult |
| Imaging | MRI useful | Stress X-rays important |
| Surgical strategy | Repair + reconstruction | Reconstruction ± osteotomy |
| Focus | Whole patient | Knee-specific evaluation |
Key Takeaways
- PLC injuries are complex but manageable with modern techniques
- Always assess vascular status and peroneal nerve function
- MRI is most useful in acute injuries
- Stress radiographs are valuable in chronic instability
- Early surgery within 7–14 days provides best results
- Repair alone has high failure rates
- Reconstruction should be combined with repair whenever possible
- Chronic varus alignment may require corrective osteotomy

Leave a Reply