Courtesy: David Chafey III, Associate Professor, University of New Mexico Health Sciences
Albuquerque, New Mexico, United States
Principles in Diagnosis and Management of Pathologic Femur Fractures
Overview
- Educational session focused on recognizing and treating pathologic femur fractures in clinical practice.
- Emphasis on systematic diagnosis, surgical decision-making, and postoperative care strategies.
Learning Goals
- Understand differences between traumatic and pathologic femur fractures.
- Recognize common causes of pathologic fractures.
- Apply a structured approach to diagnosis and treatment.
- Understand postoperative considerations and complications.
Traumatic Versus Pathologic Femur Fractures
- Traumatic fractures usually result from high-energy mechanisms and often present with associated injuries.
- Pathologic fractures frequently occur with minimal trauma or simple activities.
- Pathologic fractures often have intact periosteum and may reduce easily with traction.
- Bone healing may be impaired in pathologic fractures due to underlying disease.
Importance of Clinical History
- A detailed history is essential before reviewing imaging.
- Important factors include prior cancer history, family history of malignancy, and systemic symptoms.
- Pain preceding the fracture suggests underlying pathology.
- Medication history and comorbidities may influence management.
Common Causes of Pathologic Femur Fractures
- Metastatic disease is the most frequent cause in adults.
- Primary bone tumors are less common but important to identify.
- Metabolic bone diseases such as osteoporosis and Paget disease can lead to fractures.
- Rare disorders such as osteopetrosis may also be responsible.
Metabolic Bone Disease
- Osteoporosis is the most common metabolic cause of pathologic fractures.
- Risk factors include advanced age, chronic steroid use, smoking, and poor nutrition.
- Fractures commonly occur in the spine, distal radius, and proximal femur.
- Management includes fracture stabilization and addressing bone health.
Paget Disease
- May involve multiple bones and increase fracture risk.
- Often associated with elevated alkaline phosphatase levels.
- Surgical treatment may involve increased bleeding risk.
Diagnostic Evaluation
- Plain radiographs of the entire affected bone are essential.
- Computed tomography scans may help identify primary malignancy.
- Laboratory evaluation should include metabolic profile and calcium levels.
- Further staging depends on suspected diagnosis.
Role of Biopsy
- A biopsy is required when the diagnosis is uncertain.
- Avoid reaming through a lesion without a diagnosis.
- Frozen section examination helps guide intraoperative decisions.
- A staged procedure is reasonable if frozen section is unavailable.
Metastatic Bone Disease
- Common primary cancers include breast, lung, prostate, kidney, and thyroid malignancies.
- The axial skeleton is most commonly involved, followed by the femur.
- Metastases below the elbow and knee are rare but possible.
Treatment Objectives
- Relieve pain and restore mobility.
- Provide durable fixation with minimal need for revision.
- Allow early weight bearing whenever possible.
- Facilitate ongoing cancer treatment.
Surgical Decision-Making
- Choice of treatment depends on diagnosis, life expectancy, bone quality, and lesion location.
- Internal fixation may be appropriate when bone stock is adequate.
- Arthroplasty is preferred when fixation is unlikely to succeed.
- Cement augmentation may improve stability in destructive lesions.
Fixation Strategies
- Intramedullary nails are commonly used and should protect the entire bone.
- Plates may be useful in selected fracture patterns.
- Retrograde nails may leave proximal bone unprotected.
- Adequate reduction remains essential even in pathologic fractures.
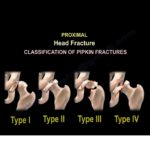
Arthroplasty Considerations
- Preferred for femoral neck fractures and severe bone destruction.
- Cemented implants often provide reliable fixation.
- Modular prostheses allow reconstruction in complex cases.
Postoperative Management
- Radiation therapy is often used for metastatic disease.
- Although radiation may delay healing, it improves pain control.
- Systemic therapy should be coordinated with oncology teams.
Complications
- Delayed union and nonunion are common due to poor bone biology.
- Implant failure may occur, especially without proper reduction.
- Infection risk may be increased in immunocompromised patients.
Special Situations
- Radiation-induced fractures may occur years after treatment.
- These fractures often require resection and reconstruction.
- Multidisciplinary care improves outcomes.
Key Takeaways
- A structured approach is essential for diagnosing pathologic femur fractures.
- Biopsy should be performed when diagnosis is uncertain.
- Surgical treatment should prioritize stability and function.
Postoperative care must address both fracture healing and underlying disease

Very nice talk