Courtesy: Amr Abdelgawad, Maimonaides Medical Centre, NY, USA
Pediatric Upper Extremity Trauma
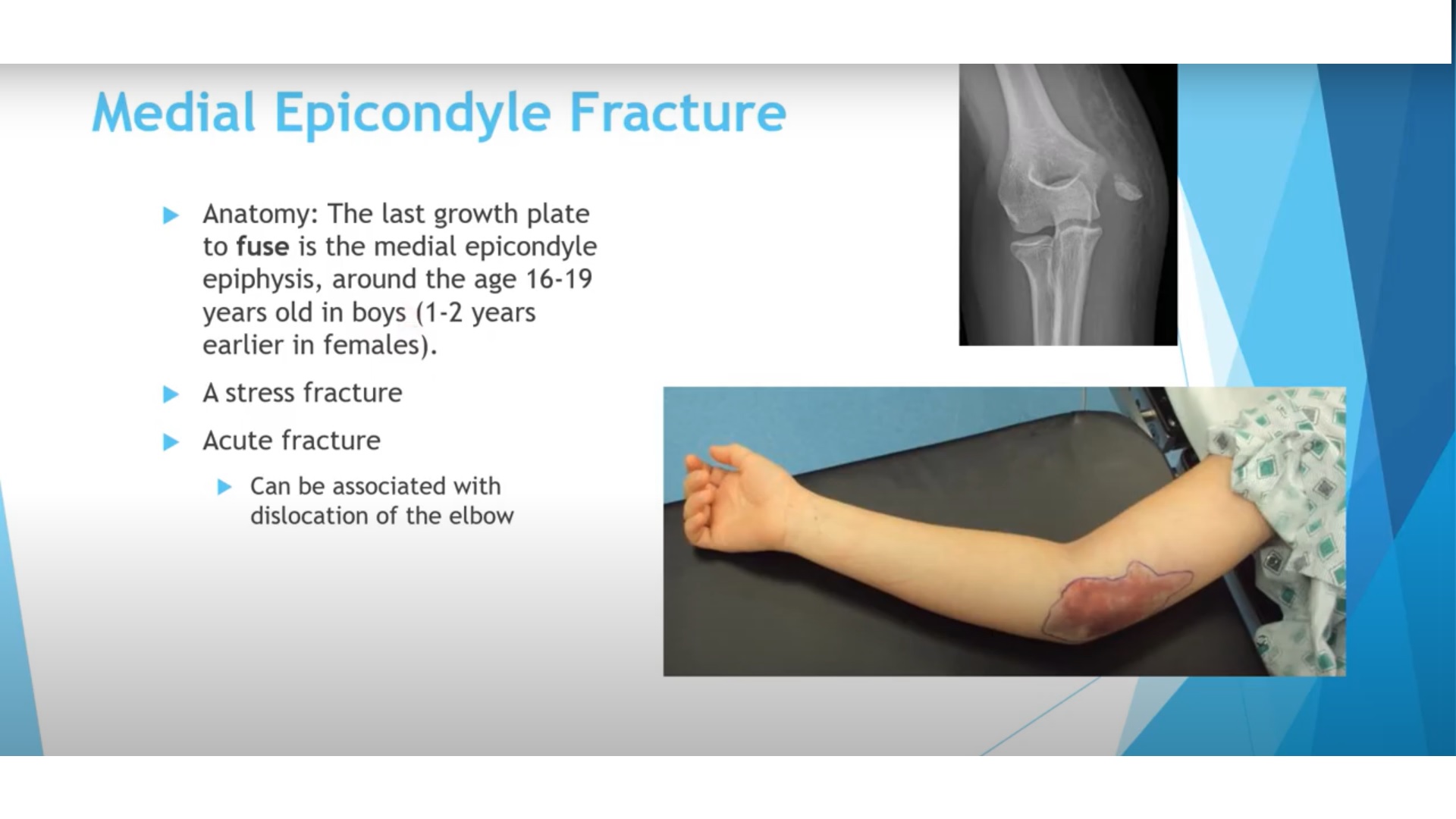
1. Medial Epicondyle Fracture (Children)
Key Anatomy
- Last ossification center to fuse in elbow
- Fusion age:
- Boys: 16–19 years
- Girls: 13–16 years
Attachments
- Medial collateral ligament (MCL)
Mechanism
- Valgus stress – avulsion injury
- Commonly associated with elbow dislocation
Treatment
Non-operative (Most Cases)
- Minimal displacement
- Stable elbow
Absolute Indication for Surgery
- Fragment entrapped in joint
Relative Indications
- Displacement >10 mm
- Valgus instability
- High-demand athletes (e.g., throwers)
2. Nursemaid’s Elbow (Pulled Elbow)
Age Group
- 2–3 years
Mechanism
- Sudden traction on a pronated forearm
Clinical Features
- Arm held:
- Pronated
- Close to body
- Refusal to move limb
- X-ray:
- Normal
Treatment
- Reduction maneuver:
- Supination – Flexion
Key Sign
- “Click” felt over radial head
- Immediate return of function
3. Radial Head & Neck Fractures (Children)
Epidemiology
- Rare
- Typical age: ~9 years
Mechanism
- Valgus force
Types
- Non-displaced
- Angulated
- Displaced
Fracture Location
- Physeal (Salter-Harris)
- Metaphyseal
Important Rule
- Radial head must align with capitellum in ALL views
Management
| Angulation | Treatment |
|---|---|
| <25–30° | Immobilization |
| >25–30° | Closed reduction |
| Persistent deformity | Percutaneous pinning |
| >45° residual | Open reduction (last resort) |
Techniques
- Closed reduction:
- Traction + supination + varus force
- K-wire joystick technique
- Metaizeau technique (intramedullary nail)
Complications
- Stiffness
- Avascular necrosis
- Radioulnar synostosis
- Non-union (rare)
4. Monteggia fracture-dislocation
Definition
- Ulna fracture + radial head dislocation
Key Clinical Rule
- Radial head must point to capitellum
Most Common Type in Children
- Bado Type I:
- Anterior radial head dislocation
- Apex anterior ulna angulation
Diagnosis Tip
- AP view may appear normal
- Lateral view is critical
Treatment
First-line
- Closed reduction of ulna
Position
- Elbow:
- 90–100° flexion
- Forearm:
- Supination
Mechanism
- Relaxes biceps – reduces radial head
If Unstable
- K-wire fixation
- Plate fixation
Missed Injury
- Ulna osteotomy + lengthening
- Radial head reduces secondarily
5. Both Bone Forearm Fractures
Incidence
- Very common pediatric injury
Acceptable Alignment
| Age | Angulation | Rotation |
|---|---|---|
| < 8 years | 15° | 45° |
| > 8 years | 10° | 30° |
Key Point
- Some shortening (overriding) is acceptable
Rotation Assessment
AP View
- Radial styloid vs bicipital tuberosity
Lateral View
- Ulnar styloid vs coronoid (180° apart)
Treatment
Conservative
- Closed reduction + long arm cast
Short Arm Cast
- For distal one-third fractures
Cast Index
- Ratio = AP / ML diameter
Normal
- < 0.8
Clinical Significance
-
0.8 – high risk of redisplacement
Surgical Indications
- Failed reduction
- Near skeletal maturity
- Unstable fractures
Surgical Options
- Flexible nails (preferred)
- Plates and screws
High-Yield Exam Pearls
- Medial epicondyle entrapped – ORIF
- Nursemaid’s elbow – supination + flexion
- Radial head must align with capitellum ALWAYS
- Monteggia = ulna fracture + radial head dislocation
- Missed Monteggia – ulna osteotomy
- Cast index < 0.8
- Distal radius – high remodeling potential
Critical Warning
- Avoid open reduction in radial neck fractures:
- Higher complication rates
Final Message
- Pediatric upper limb trauma requires:
- Accurate anatomical understanding
- Careful radiographic assessment
- Preference for conservative treatment when possible
to ensure optimal functional outcomes


Leave a Reply