Courtesy: Prof Shital Parikh, Professor, Cincinatti Childrens Hospital, Cincinatti, Ohio, USA
Pediatric ACL Tears & Tibial Spine Fractures – High-Yield Notes
Pediatric ACL Tear
Natural History (IMPORTANT)
- Non-operative – poor outcomes
- instability
- meniscal tears
- return to sports
- Delay > 12 weeks – irreparable meniscus injury
Conclusion: Early surgical management preferred
Assessment of Skeletal Maturity
Methods:
- Tanner staging (unreliable clinically)
- Bone age (hand X-ray)
- Distal phalangeal physis:
- Open >2 years growth remaining
- Closing <2 years growth
? Treatment Algorithm (VERY IMPORTANT)
- Prepubescent (Tanner I–II)
- Age: ~8–10 years
- Physeal-sparing (Extra-articular)
- Iliotibial band technique (MacIntosh)
- Intermediate (Growth remaining >2 yrs)
- Epiphyseal ACL reconstruction
- Tunnels within epiphysis (no physis violation)
- Near maturity (<2 yrs growth)
- Transphyseal ACL reconstruction
- Principles:
- Tunnel < 8 mm
- Physeal damage < 5%
- Soft tissue graft
- Avoid hardware across physis
- Principles:
Graft Choices
- Preferred: Hamstring / Quadriceps tendon
- Avoid: Allograft ( failure in children)
Return to Sports
- Minimum: 6 months
- Preferred: 9–12 months
- Add:
- Functional testing
- ACL brace (select cases)
- Injury prevention programs
Complications
- Growth disturbance (rare ~1.3%)
- Valgus deformity
- Limb length discrepancy
- Re-tear rate higher than adults
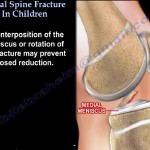
Tibial Spine (ACL Avulsion) Fracture
Classification (Meyers & McKeever)
- Type I – Undisplaced
- Type II – Hinged
- Type III – Completely displaced
- Type IV – Comminuted
Management
Type I
- Casting
Type II–IV
Surgical fixation (preferred)
Why Not Conservative
- Meniscal interposition common
- Malunion extension block
- High arthrofibrosis risk with immobilization
Fixation Options
- Screw fixation
- Strong fixation
- Requires removal later
- Suture fixation
- No second surgery
- Useful in comminuted fractures
Outcomes: No major difference
Surgical Principles
- Anatomical reduction
- Rigid fixation
- Early mobilization (to prevent stiffness)
Complications
Most important: Arthrofibrosis
- Prevention:
- Early surgery
- Early ROM
- Stable fixation
Others:
- Residual laxity (due to ACL stretch)
- ~5–20% may need later ACL reconstruction
Important Clinical Pearls ?
- Distal femur physis contributes:
- 70% femoral growth
- 37% limb growth
- ACL avulsion always normal ACL
May lead to future instability - In children:
Treat ACL early, don’t wait for maturity
One-line Summary
- Pediatric ACL early surgery + growth-respecting technique
- Tibial spine fracture fix displaced, mobilize early


Leave a Reply