Courtesy:Dr Amr Abdelgawad, Associate Professor, University of Texas, USA
www.facebook.com/pediatricorthopedic
Non-accidental trauma (NAT) – Orthopaedic Perspective
Definition
- Non-accidental trauma (NAT):
- Injury intentionally inflicted or due to neglect
- Previously referred to as:
- Child abuse
Epidemiology
- Occurs in ~1–1.5% of children annually
- Significant global burden
Key Demographic
- Most common in:
- Children < 3 years of age
Risk Factors
- Age < 3 years
- Firstborn child
- Prematurity
- Disabled child (e.g., cerebral palsy)
- Stepchildren
- Single-parent families
- Parental history of abuse
Clinical Red Flags (Most Important Section)
A. History
- Inconsistent or changing history
- Mechanism does not match injury
- Different stories to different doctors
- Delay in seeking treatment
B. Caregiver Behavior
- Indifferent
- Hostile
- Unconcerned attitude
Fractures Highly Suggestive of NAT
Very High Suspicion
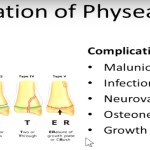
- Metaphyseal (corner / bucket-handle) fractures
- Distal femur
- Proximal tibia
- Rib fractures
- Especially posterior ribs
- Distal humerus transphyseal fractures
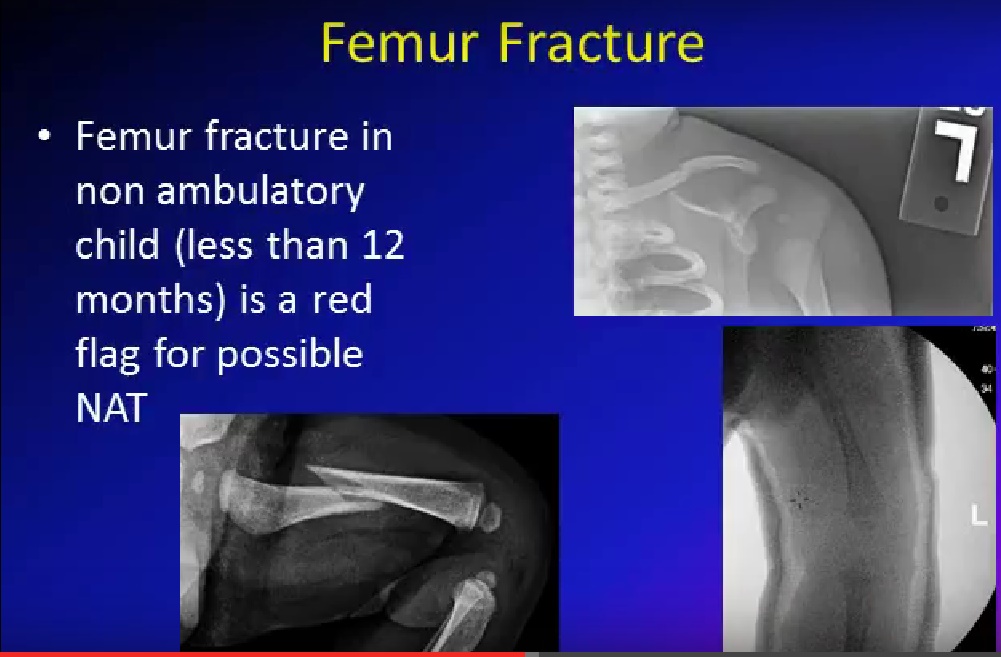
High Suspicion
- Femur fracture in:
- Child <1 year
- Non-ambulatory child
- Humerus shaft fracture:
- <3 years
Other Suspicious Findings
- Fractures in different stages of healing
- Bilateral fractures
- Finger fractures in non-ambulatory child
- Complex skull fractures
Important Exam Concept
Myth
- Spiral fracture = abuse
Reality
- Spiral fractures occur in:
- Both accidental and non-accidental trauma
- Only ~1/3 NAT fractures are spiral
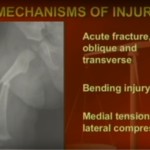
Characteristic Injury Patterns
1. Metaphyseal (Corner) Fractures
- Highly specific for abuse
- Mechanism:
- Shearing / pulling forces
2. Rib Fractures
- Posterior ribs most common
- Mechanism:
- Chest compression
3. Femur Fracture
- Red flag if:
- <1 year
- Non-ambulatory
4. Multiple Fractures
- Different healing stages – repeated injury
5. Periosteal Reaction
- Suggests healing injury
- May be:
- Extensive
- Multifocal
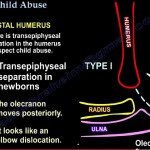
6. Transphyseal Distal Humerus Fracture
- Mechanism:
- Twisting / traction
Key Feature
- Radius & ulna not aligned with humerus
Diagnosis
- Difficult (cartilage not visible on X-ray)
- Confirm with:
- MRI
- Arthrogram
Investigations
1. Skeletal Survey (Most Important)
Includes:
- Skull (AP + lateral)
- Spine
- Chest
- Pelvis
- Long bones
- Hands & feet
If negative but suspicion persists:
- Repeat after 1 week
2. Bone Scan
- Useful when skeletal survey is negative
- Better for:
- Rib fractures
- Vertebral injuries
3. CT / MRI
- For:
- Complex injuries
- Transphyseal injuries
Management
Principles
- Detailed history
- Correlate injury with mechanism
- Maintain high suspicion
Steps
- Involve child protection services early
- Inform primary physician
- Admit child if safety is uncertain
- Treat fractures per orthopaedic principles
Differential Diagnosis
(Not all fractures = abuse)
- Accidental trauma
- Osteogenesis imperfecta
- Rickets
- Metabolic bone disease
- Osteomyelitis
- Physiological periostitis
Legal Aspect
- Mandatory reporting if suspected
- Clinician is protected if reporting:
- Done in good faith
Exam Pearls (High-Yield)
- Most specific fractures:
- Metaphyseal + rib fractures
- Most important clue:
- Inconsistent history
- Red flag:
- Fracture in non-ambulatory child
- Classic finding:
- Multiple fractures in different stages
- MCQ trap:
- Spiral fracture not always abuse
Final Clinical Message
- Always correlate:
- History + injury pattern + child’s developmental stage
- Missing NAT can lead to:
- Recurrent injury
- Severe morbidity or mortality
Leave a Reply