Courtesy: Prof Nabile Ebraheim, University of Toledo, Ohio, USA
Introduction
-
Myositis ossificans is currently more accurately termed heterotopic ossification.
-
It is a reactive, non-neoplastic lesion occurring in soft tissues.
-
The condition is characterized by fibrous tissue proliferation, followed by cartilaginous and osseous metaplasia.
-
The entity was first described in 1883 by Riedel.
-
The terminology is derived from Greek:
-
Hetero meaning other
-
Topos meaning location
-
Ossificans meaning bone formation
-
Types of Heterotopic Ossification
-
Genetic forms (rare)
-
Non-genetic forms (most common)
Classification Based on Etiology
-
Neurogenic heterotopic ossification
-
Traumatic heterotopic ossification
-
Fibrodysplasia ossificans progressiva (also known as Munchmeyer disease)
Classification Systems
Brooker Classification
-
Presence of isolated islands of bone within soft tissues
-
Bone spurs arising from the pelvis or proximal femur with a gap greater than one centimeter between opposing surfaces
-
Bone spurs with opposing surfaces separated by less than one centimeter
-
Complete bony ankylosis of the joint
Della Valle Classification
-
Includes the first three grades of the Brooker classification
-
Does not include complete ankylosis
Etiology and Pathogenesis
-
Heterotopic ossification represents aberrant tissue repair following surgery or traumatic insult.
-
The process may be triggered by immobilization or external stimuli.
-
Injury to soft tissues around a joint or long bone leads to:
-
Influx of inflammatory cells
-
Release of signaling molecules
-
Activation of mesenchymal stem cells
-
-
These cells undergo osteogenic or osteochondrogenic differentiation.
-
Bone formation occurs through membranous or endochondral ossification pathways.
Anatomical Locations
Heterotopic ossification may develop in:
-
Skeletal muscles
-
Fascia
-
Tendons
-
Ligaments
-
Subcutaneous tissue
-
Skin
-
Vessel walls
-
Any site containing connective tissue
Epidemiology
-
Most commonly affects young adults.
-
Male to female ratio is approximately 3:2.
-
Frequently associated with a prior insult such as:
-
Trauma
-
Surgery
-
Repeated massage
-
Common Associated Conditions
-
Hip arthroplasty (approximately 40 percent)
-
Bone fracture or joint dislocation (approximately 30 percent)
-
High-energy extremity trauma
-
Traumatic brain injury
-
Spinal cord injury (up to 50 percent)
-
Neurological disorders
-
Severe burns
When to Suspect Heterotopic Ossification
-
History of trauma, surgery, or forceful massage
-
Progressive stiffness around a joint
-
Stiffness at common sites of injury such as:
-
Elbow
-
Hip
-
Pelvis
-
Knee
-
-
Association with autoimmune conditions such as dermatomyositis or systemic sclerosis, where skin involvement is common
Clinical Presentation
Early Inflammatory Phase
-
Localized pain
-
Tenderness
-
Swelling
-
Rapid increase in size of the lesion
Maturation Phase
-
Progressive maturation of bone tissue
-
Lesion becomes firm and well localized
-
Increasing restriction of joint movement
Investigations
Plain Radiographs
-
No visible ossification in early stages
-
Early lesions may show ill-defined soft tissue opacities without clear zonal maturation
-
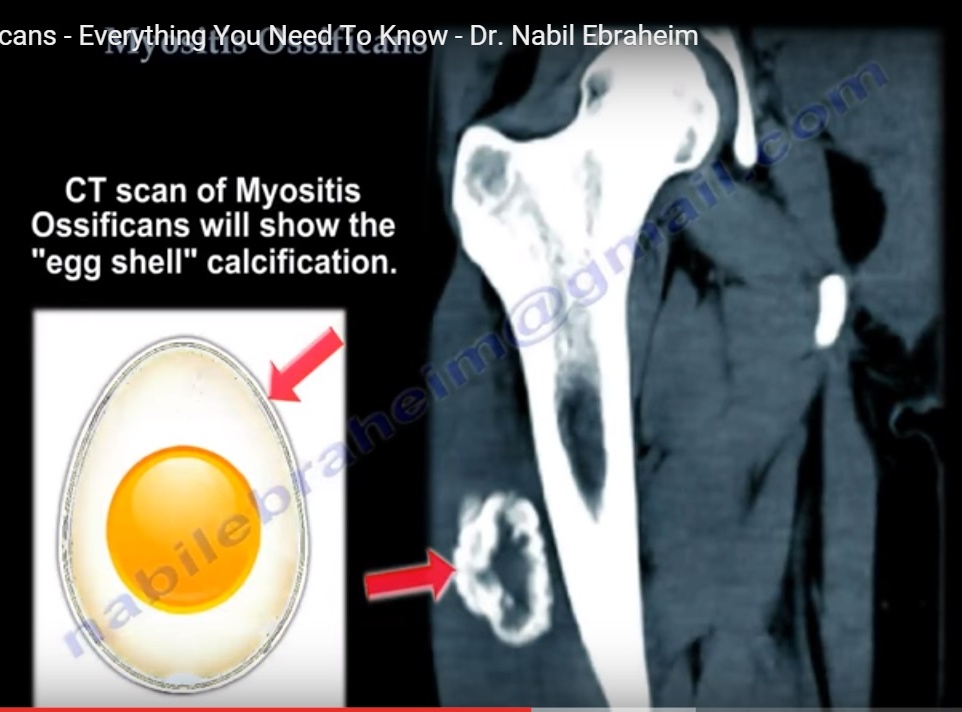
Mature intramuscular heterotopic ossification shows:
-
Well-demarcated radiodense mass
-
Peripheral ossification with central lucency
-
Typical “eggshell” pattern of calcification
-
-
Lesions usually involve soft tissue alone
-
When attached to the bone surface, the condition is termed parosteal heterotopic ossification:
-
Initially seen as a narrow stalk
-
Later develops a broad bony attachment with cortical continuity
-
-
Advanced stages may show joint ankylosis
Computed Tomography
-
Best modality to demonstrate zonal maturation.
-
Early lesions appear as low-density soft tissue masses.
-
Follow-up imaging demonstrates peripheral ossification.
-
Useful for assessing proximity to neurovascular and other vital structures.
Magnetic Resonance Imaging
-
Appearance varies with stage of maturation.
-
Early lesions show:
-
Ill-defined mass
-
Heterogeneous signal intensity
-
Surrounding soft tissue edema
-
Possible fluid-fluid levels due to hemorrhage
-
-
Contrast-enhanced imaging shows central enhancement due to vascularity.
-
Mature lesions demonstrate peripheral rim enhancement.
-
Key distinguishing feature:
-
Heterotopic ossification shows central vascularity with peripheral ossification
-
Malignant sarcomas show central ossification with peripheral vascularity
-
Positron Emission Tomography
-
Usually performed in combination with computed tomography.
-
Uses radiolabeled fluoride or radiolabeled glucose.
-
Radiolabeled fluoride binds to hydroxyapatite and detects early bone formation.
-
Useful for identifying metabolically active lesions.
Histopathology
-
Early lesions are hypercellular with spindle-shaped cells and minimal bone matrix.
-
May resemble nodular fasciitis or granulation tissue.
-
Findings include:
-
Mitotic figures
-
Multinucleated giant cells
-
Inflammatory infiltrate
-
Extravasated red blood cells
-
-
With maturation:
-
Zonal architecture becomes evident
-
Peripheral woven bone with osteoblastic rimming develops
-
-
Gradual transition from woven bone to mature lamellar bone distinguishes heterotopic ossification from osteosarcoma.
-
Mature lesions show:
-
Well-circumscribed mass
-
Fibrous pseudocapsule
-
Thick-walled blood vessels
-
Lamellar bone with fatty marrow
-
Presence of Haversian systems and Volkmann canals
-
Differential Diagnosis
-
Parosteal osteosarcoma
-
Soft tissue sarcomas, including malignant fibrous histiocytoma
-
Synovial sarcoma
Management
Prophylaxis
-
Radiation therapy
-
Non-steroidal anti-inflammatory drugs
Radiation Therapy
-
Used prophylactically after hip arthroplasty in high-risk patients such as those with:
-
Ankylosing spondylitis
-
Diffuse idiopathic skeletal hyperostosis
-
Hypertrophic osteoarthritis
-
Prior history of heterotopic ossification
-
-
Typical dose ranges between 400 and 700 centigray.
-
Potential adverse effects include joint stiffness.
-
Long-term oncogenic risk remains controversial and requires cautious use.
Non-Steroidal Anti-Inflammatory Drugs
-
Indomethacin administered at 25 milligrams three times daily for six weeks has been shown to reduce heterotopic ossification formation.
-
Gastrointestinal irritation and gastritis are recognized complications.
Surgical Management
-
Surgery should only be performed after complete maturation of the lesion.
-
Early excision increases the risk of recurrence.
-
Challenges include:
-
Poorly defined tissue planes
-
Encasement of neurovascular structures
-
Incomplete excision leading to recurrence
-
-
Full maturation may take six months or longer, during which joint ankylosis may occur.
-
Acceptable functional outcomes have been reported even in ankylosed joints.
Neurogenic Heterotopic Ossification
-
First described in 1918 by Dejerine and Ceillier in patients with spinal cord injury during the First World War.
-
Common sequela of spinal cord injury.
-
Also associated with:
-
Traumatic brain injury
-
Stroke
-
Hypoxic encephalopathy
-
Encephalitis
-
Tetanus
-
Poliomyelitis
-
Syringomyelia
-
Burns
-
-
Develops between three and twelve weeks after injury.
-
Bony injury is not required for development.
-
More common in complete spinal cord injuries.
-
Occurs below the level of neurological injury.
-
Hip is the most frequently affected joint.
-
Often extensive and may involve multiple sites.
Fibrodysplasia Ossificans Progressiva
-
Rare, slowly progressive genetic disorder.
-
Inherited in an autosomal dominant pattern, usually due to spontaneous mutation.
-
Caused by mutation in the ACVR1 gene, most commonly the R206H mutation.
-
Leads to excessive bone morphogenetic protein signaling and endochondral ossification.
-
Presents in early childhood.
Clinical Features
-
Progressive ossification of muscles, tendons, and ligaments
-
Severe joint stiffness and loss of mobility
-
Disease spreads from:
-
Neck and shoulders
-
Trunk
-
Limbs
-
-
Temporomandibular joint involvement causes difficulty with eating and speech.
-
Most patients become wheelchair-bound by early adulthood.
-
Diaphragm, tongue, and extraocular muscles are spared.
Skeletal Abnormalities
-
Congenital malformation of the great toe
-
Hallux valgus deformity
-
Clinodactyly
-
Short and broad femoral necks
-
Costovertebral joint ankylosis
-
Intercostal muscle ossification
-
Sensorineural and conductive hearing loss
Atypical Fibrodysplasia Ossificans Progressiva (FOP Plus)
-
Involvement of head and neck with sparse scalp hair
-
Cognitive impairment and seizures
-
Cranial and cerebral malformations
-
Ocular abnormalities including cataracts and glaucoma
-
Additional skeletal disorders
-
Endocrine and hematological abnormalities
-
High mortality due to restrictive lung disease, pneumonia, malnutrition, or right-sided heart failure
-
Median life expectancy is approximately forty years
-
Pregnancy carries high maternal and fetal risk
Treatment of Fibrodysplasia Ossificans Progressiva
-
No definitive curative treatment exists.
-
Surgical excision worsens disease progression.
-
Short courses of corticosteroids during flare-ups may provide limited benefit.
-
Etidronate and non-steroidal anti-inflammatory drugs may help symptom control.
Preventive Strategies
-
Lifestyle modification to minimize trauma
-
Avoidance of contact and impact sports
-
Household safety measures to prevent falls
-
Respiratory physiotherapy to prevent pulmonary complications
Progressive Osseous Heteroplasia
-
Rare genetic disorder
-
Caused by inactivating mutations in the GNAS1 gene
-
Inherited in an autosomal dominant pattern
-
Presents with dermal ossification in childhood
-
Progresses to deep connective tissue and skeletal muscle involvement
Albright Hereditary Osteodystrophy
-
Genetic syndrome with multiple systemic manifestations
-
Short stature and obesity
-
Rounded facial features
-
Subcutaneous ossifications
-
Shortening and widening of metacarpals and metatarsals, especially the fourth and fifth rays
-
Temporomandibular joint ankylosis
Leave a Reply