Courtesy: Prof Nabil Ebraheim, University of Toledo, Ohio, USA
Metatarsal Fractures
Metatarsal fractures can involve:
-
First metatarsal
-
Fifth metatarsal
-
Second, third, and fourth metatarsals (including stress fractures)
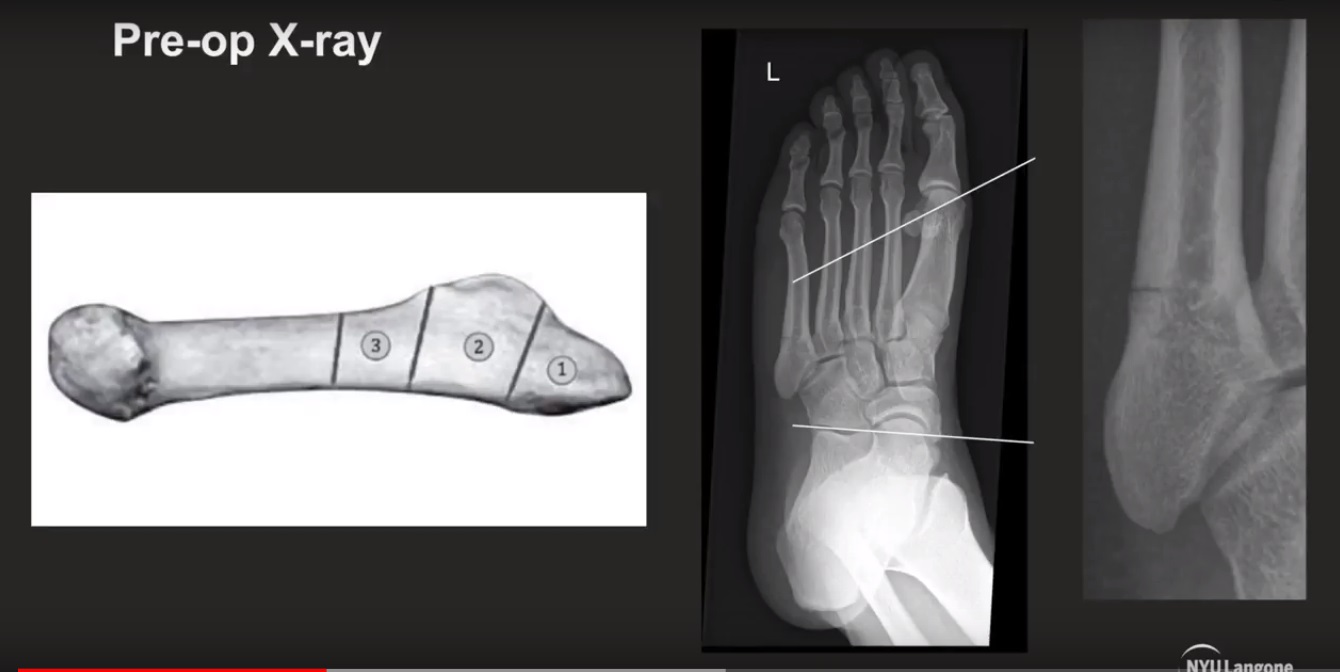
1. First Metatarsal Fractures
Key Points
-
Different from fractures of the second, third, and fourth metatarsals.
-
The first metatarsal carries a greater load.
-
Malunion may cause:
-
Transfer lesions
-
Uneven weight distribution.
-
Management
-
Aim for perfect alignment and fixation.
-
More likely to require:
-
Open reduction
-
Internal fixation (ORIF)
-
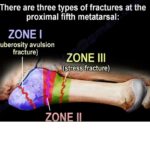
2. Fifth Metatarsal Fractures
Jones Fracture (Zone 2)
-
Occurs in a vascular watershed area.
-
Located in the proximal fifth metatarsal.
-
Often enters the fourth and fifth intermetatarsal articulation.
-
Healing may be difficult without surgery.
Management
-
Commonly treated with screw fixation in:
-
Athletes
-
Young active individuals
-
-
Percutaneous intramedullary screw fixation:
-
Typically a 4.5 mm screw
-
Offers shortest time to union
-
Lowest risk of nonunion
-
Allows early return to activity.
-
Surgical Risk
-
Sural nerve injury is a risk during intramedullary screw fixation.
Nonoperative Treatment
-
Casting and non-weight bearing acceptable if:
-
Acute fracture
-
Non-displaced.
-
-
Risk of recurrent fracture after nonsurgical healing: approximately 30%.
Zone 1 Fracture (Pseudo-Jones)
-
Enters the tarsometatarsal joint (metatarsocuboid joint).
-
Treated conservatively.
-
Initiate weight-bearing as tolerated.
-
Use fracture shoe.
-
Heals well.
-
Less serious than Zone 2 and Zone 3 fractures.
Zone 3 Fracture
-
Proximal diaphyseal fracture distal to the fourth and fifth articulation.
Shaft Fractures of the Fifth Metatarsal
-
Treated with:
-
Weight-bearing
-
Walking cast
-
Walking boot
-
Midfoot Injuries
-
Maintain high suspicion for associated injury to:
-
Tarsometatarsal joint (Lisfranc joint).
-
-
Obtain:
-
Standing X-rays
-
Stress X-rays
-
-
Rule out Lisfranc injury.
3. Second Metatarsal Fractures
Stress Fracture in Ballet Dancers
-
Common at the base of the second metatarsal.
March Fractures
-
Occur in:
-
Second metatarsal
-
Third metatarsal.
-
Clinical Presentation
-
Forefoot pain
-
Swelling
-
No history of trauma
-
Tenderness along the metatarsal shaft
Treatment
-
Protected weight-bearing
-
Walking boot
-
Walking cast
Summary
-
First metatarsal fractures require accurate fixation due to load-bearing role.
-
Jones fractures (Zone 2) have higher risk of nonunion and often require surgical fixation in active patients.
-
Zone 1 fractures heal well with conservative treatment.
-
Always rule out Lisfranc injury in midfoot trauma.
-
Stress fractures commonly involve the second and third metatarsals and are treated conservatively

Leave a Reply